











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkINTRODUCTION
Chronic kidney disease is associated with several consequences at different levels: physical, psychological, and socio-economic (1) and it is considered a source of stress and a significant public health problem (2).In Spain, kidney transplantation is the treatment of choice in the majority of cases (3). However, it is a complex treatment that requires the person to make lifestyle changes (4,5). Hence, this type of intervention can generate psychological complications (6) with repercussions on the quality of life (QoL) (7).The concept of QoL involves biological, psychological, and social factors which from a subjective and objective perspective, are related to the individual's satisfaction with life (8). According to the literature, poor QoL is closely related to the appearance of morbidity and early mortality (9,10).The World Health Organization (WHO) defines QoL as an individual's perception of their position in life in the context of the culture and value systems in which they live and regarding their goals, expectations, standards, and concerns. It is a broad-ranging concept affected in a complex way by the person's physical health, psychological state, level of independence, social relationships, personal beliefs, and their relationship to salient features of their environment (11).Numerous scales exist to assess QoL, the Kidney Transplant Questionnaire (KTQ) is economical, simple, and easy to use (12).Several studies have shown an association between a worse QoL and anxiety (13,15). The questionnaire State-Trait Anxiety Inventory (STAI) rates overall anxiety, discriminating between anxiety as an inherent feature of a person and the transient anxiety that is caused by some stress factor. Today, our society faces a worldwide crisis caused by the rapid propagation of SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) (16). The first case was confirmed in Spain on January 31, 2020, and the disease was classified as a pandemic on March 11 of that same year by the WHO (17).The recipients of a kidney transplant are a vulnerable population because of their situation of immunosuppression or because of the high prevalence of comorbidities, such as arterial hypertension, diabetes, or cardiovascular disease (18,20).Taking into account the background, this study aims to explore the incidence of anxiety and perceived QoL in people with a kidney transplant who tested positive for coronavirus versus those who did not, in addition to determine the incidence of cases and deaths due to SARS-CoV-2 in the study population.
MATERIALS AND METHODS
As no prior data on this topic are available, this was a retrospective exploratory study of prospective cohorts.
Candidates were included in this study if they were older than 18 years, had a kidney transplant, and were under follow-up at the Kidney Transplant Outpatients Clinic in a tertiary teaching hospital, in Spain. Exclusion criteria were residents of another autonomous community, those unable to give their written consent, those not willing to participate, and those unable to adequately speak Spanish and/or read in Spanish.
The targeted population for the first cohort (cases) was selected including data for all individuals with a kidney transplant who had tested PCR-positive or antigen test positive for SARS-CoV-2 during what is known in Spain as the second wave (July 1 to December 5, 2020) of the pandemic, who did not need to be admitted to hospital during the period in question and irrespective of whether they presented COVID symptoms or not. The dates of the waves were as described by the Spanish Ministry of Health (21). In this way, we tried to minimize the memory bias related to too much time after having the infection. For the second cohort (not-cases), we recruited a similar number of consecutive individuals from the target population who had not suffered the virus infection.
In some of the data for the second pandemic wave, the outcome variables determined were: anxiety, QoL, and death. The following were the independent variables recorded: SARS-CoV-2 infection, sex, age, transplant duration, cause of death, education level, number of co-habitants at home, civil state, and yearly income.
To measure the level of anxiety, we used the Spanish adaptation of the STAI questionnaire, which was self-administered (22,24). The scale consists of 20 sentences through which the subject can describe how they feel at a particular moment, in this case, when they were suffering from COVID-19, and another 20 sentences to describe how they felt in general, using Likert responses from 0 to 3.
In the final result, scores are obtained for the state of anxiety and for the type of anxiety by adding the items of each dimension. The score can vary between 0 and 60 with no defined cut-off points but given that the highest values indicate a high level of anxiety, the following cut-off points were established: 0 to 10 - a low level of anxiety, 11 to 29 - a medium level of anxiety, 30 and above - a high level of anxiety (23).
The reliability of this questionnaire is estimated with a Cronbach alpha coefficient above 0.8 in all dimensions (24).
To assess QoL as perceived by the subject, the Spanish version of the KTQ questionnaire was self-administered (25). This is a questionnaire specifically for patients with a functioning kidney transplant which provides information on the physical extent (with the dimensions “Physical symptoms” and “Fatigue”) and the psychological extent (via the dimensions “Uncertainty/Fear”, “Appearance” and “Emotions”). Likert responses from 1 to 7 were used, with a reference period of two weeks.
The reliability of this questionnaire is estimated with a Cronbach alpha coefficient above 0.70 in all dimensions except for “Appearance”, with a Cronbach alpha of 0.69 (25).
In a descriptive analysis, qualitative variables are provided as their frequency distributions and quantitative variables as the mean and standard deviation if showing a normal distribution. When this was not the case, they were expressed as their median and interquartile range (IQR).
Between groups, qualitative variables were compared using the Chi-square test, or Fisher's exact test when more than 25% of expected frequencies were under 5. To compare quantitative variables, we used the student t-test, or Mann-Whitney U test when these were not normally distributed.
To correct for possible confounding factors, we constructed logistic regression models with the main outcome measure such that all variables were included in a stepwise procedure in a linear regression model.
All scales were considered dependent variables and the rest of the variables were considered independent variables. Significance was set at a p <0.05 (two-tailed). All statistical tests were performed using the software package IBM SPSS Statistics v21.
The study protocol was approved by the Ethics Committee on Healthcare Research of the Hospital Clínico San Carlos (reference 20/816-E), Madrid, Spain.
RESULTS
The study participants were 601 kidney transplant recipients with a mean age of 61.7 years (SD 12.8) of whom 61.9% (n= 372) were men. The median transplant duration was 10 years (IQR: 5-15).
From the start of the pandemic until the end of the second wave, 12.1% (n=73) suffered SARS-CoV-2 infection and 6.2% (n=37) deaths were recorded: 3 of unknown cause, and 52.9% (n=18) of the remaining individuals (n=34) died of coronavirus infection. These figures translate to a mortality rate of 2.9% and a case fatality rate of 24.7%.
Looking at the mortality data from the first wave, it was found that 13 of 36 infected persons died, translating to a mortality of 6% and case fatality of 36.1%, in contrast during the second infection wave, 6.2% (n=37) of the study population were infected with SARS-CoV-2 and 5 people died, all as the consequence of coronavirus infection, determining mortality of 0.8%, and case fatality of 13.5%.
Significant differences were detected in death and lethality rates (p< 0.000) between those who had had the infection and not during the second wave.
To conduct the structured interview, we tried to contact all those infected by SARS-CoV-2 during the second wave in our study population (n=28). Among these individuals, we were able to interview 22, such that the response rate was 78.6%. The mean age of these subjects (n=22) was 55.1 years (SD 11.1) and 50% (n=11) were men.
For the not-cases cohort, 36 individuals (n=36) of those who had never tested positive for SARS-CoV-2, were selected for interview by consecutive sampling at the nursing facility of the Kidney Transplant Outpatients Clinic. The mean age of this cohort was 57.9 years (SD 14.2); 63.9% (n=23) were men.
After carrying out the interview, the individuals were given the questionnaire, which they completed themselves in a room made available for this purpose. Both the interview and the questionnaire were carried out in the framework of a visit to the Kidney Transplant Outpatients Clinic.
The sociodemographic characteristics of the subjects interviewed are provided inTable 1.
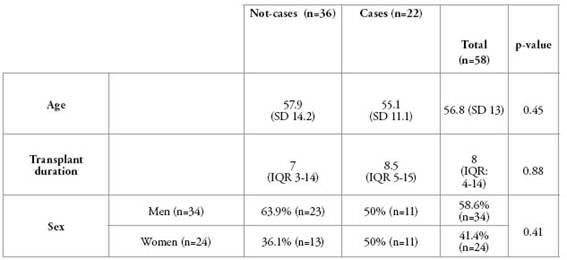
TABLE 1: Sociodemographic characteristics of the study population.
No significant differences were found in sex, age, kidney transplant duration, civil state, yearly income or education level between those with and without coronavirus (p >0.05).
58 individuals completed the KTQ, but one was eliminated because the replies given were similar for all questions. QoL was 4.1 (SD 0.9) for the whole population, 4 in 51.4% of the cases and 54.5% in the not-cases, with no significant difference between them (p= 0.87). The results are provided inTable 2.
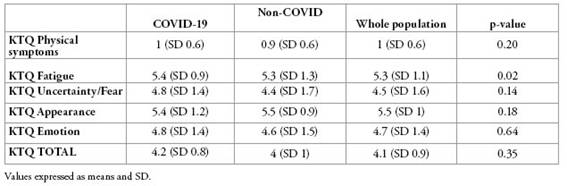
TABLE 2: Scores obtained in each dimension of the KTQ.
Significant differences were found when relating QoL scores with descriptive variables in the case and not-cases cohorts.
Among the not-cases, significant differences emerged in age. Thus, Pearson's correlation coefficient revealed that age had an effect, albeit small, on overall QoL and in the score awarded to the dimension Uncertainty/Fear (r=0.214 and 0.22 respectively), while a greater effect of age was observed on Appearance (r=0.532). This meant that the older a person ages, the better the life quality as measured in terms of this factor. In this cohort, the number of coinhabiting family members also had a significant impact on life quality in terms of Emotion (p=0.03).
In the cohort cases, it was found that the effect of age in the dimension Fatigue was moderate (r= 0.370) while in terms of Uncertainty/Fear (r= 0.401), Appearance (r= 0.703), Emotion (r= 0.449), and overall life quality (r= 0.539), the effect of age was large, the older the person, the better being QoL. In addition, significant differences were also observed in life quality in terms of Fatigue according to income (p= 0.019).
In the STAI, 58 interviews were conducted, and valid replies were obtained for 57 participants (Table 3).

TABLE 3: Scores obtained for each STAI subsection.
In 63.6% of cases, anxiety-state scores were greater than 40, versus 82.4% in the not-cases group. Scores for anxiety traits higher than 40 were recorded in 63.6% compared to 79.4% of the cases versus not-cases, respectively. These differences were nevertheless not significant (Table 3).
According to the literature (23), the levels of anxiety of our study sample may be categorized as detailed inTable 4.
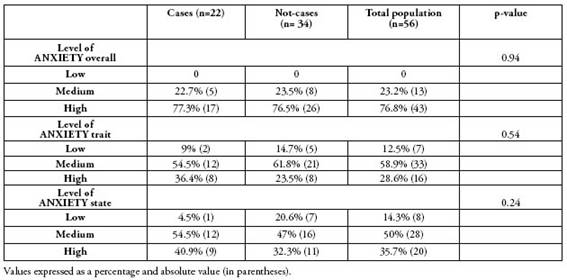
TABLE 4: Scores recorded for all categorized subsections of STAI.
Anxiety levels were found to be affected by age. In the not-cases cohort, age had a mild effect on Anxiety-state (r= 0.142), Anxiety-trait (r= 0.278), and Anxiety-overall (r= 0.211) such that the older the person, the greater the level of anxiety. While in the cases, the effect of age on Anxiety-trait was moderate (r= -0.396), this effect was greater when we considered Anxiety-state (r= -0.511) or overall anxiety (r= -0.467). In these subjects, the older the person, the lower the level of anxiety overall, and also of trait and state anxiety.
No significant differences between cohorts were detected in anxiety levels when analyzing the remaining descriptive variables.
DISCUSSION
This study sought to assess the impacts on anxiety and QoL of having experienced coronavirus infection in persons with a kidney transplant (26).
The results indicate that the two cohorts were homogeneous in terms of sociodemographics.
Our results also indicate that SARS-CoV-2 affected a large proportion of our study population (12.1%). This rate is in line with the figure of 11.7% provided by a seroprevalence study conducted in the general population of Spain (Gobierno de España. Ministerio de Sanidad. Consejo Interterritorial Sistema Nacional de Salud. Instituto de Salud Carlos III, 2020).
At the time of writing, no estimates were found of the overall incidence of SARS-CoV-2 infection in individuals with a kidney transplant. However, some reports do exist of cases or case series (28); of studies that do not specify the target population (29,30); of those considering very specific kidney transplant populations such as one detecting an incidence of 9% in patients receiving a kidney in the last 60 days (31); or of studies with very short follow-up duration such as one (32) that described an incidence of 0.2% for 1 month of follow up.
When trying to compare populations from different countries, we need to be cautious as the virus has affected different regions very differently. It should be therefore taken into account that at the start of the pandemic, Spain was among the three most affected countries, Madrid being an epicenter of the disease (33).
The mortality rate recorded here for the period encompassing the two first waves of the pandemic was low (2.9%) compared to the rates reported by others for kidney transplant recipients in Spain, which are in the range of 21%27 to 43% (29). Unlike our participants who were under ambulatory follow-up, the populations examined in these studies were mainly hospitalized patients, suggesting they were probably more severe cases of coronavirus. In the second wave, the 0.8% obtained approaches the 1% reported for the general population of the Comunidad de Madrid for the same period (34).
The case fatality rate recorded over the first two waves of infection was high (24.7%), more than doubling the rate of 11.3% reported for the general population (34). However, our rate is in line with those provided for the Spanish series of kidney transplant recipients which range from 21% (28) and 26.8% (29) to 33% (35).
Our study provides new information on mortality and case fatality, in individuals with a kidney transplant under ambulatory follow-up. The study was designed to avoid Berkson's selection bias (36).
The data obtained about self-reported QoL failed to differ significantly between subjects with and without coronavirus infection both in terms of overall scores or any dimension except Fatigue. We envisaged that our study could provide useful information to identify the psychological care needs of patients followed at the Kidney Transplant outpatient facility.
Mean QoL scores for the two cohorts separately and together indicate that individuals with a kidney transplant have only a moderate level of emotional well-being.
These data are consistent with those reported in the literature for kidney transplant recipients. For example, in a study conducted in Palestine (37), the mean QoL score was 4.02 (SD 0.8), and Appearance was the dimension awarded the higher score (5.4 SD 1.23), as observed here. Higher scores were obtained in another study performed in a Spanish population (25), and while QoL scored a mean of 5.5, body appearance was scored highest and physical symptoms lowest, coinciding with the present results.
The effect of sex on perceived QoL seems to vary widely. International studies have also noted no difference in QoL scores related to sex (37,39). However, others have found that in men, self-reported QoL is significantly higher than in women (40).
In our study, age had an impact on QoL depending on whether the individual had had coronavirus infection or not, such that the older a person, the better this dimension of QoL. We feel this could be the consequence of older persons being more resilient and better able to accept any physical changes caused by their underlying disease, although there is no evidence of this in the literature.
A large proportion of our study population, 76.8%, reported they had a high level of anxiety. This figure is much higher than that described for other populations. According to the results of a meta-analysis on the general population (41), the prevalence of anxiety was 31.9%, while another study provided a rate of 33.9% for kidney transplant recipients (42), that is, less than half the level recorded in the present study. In effect, poor health has been identified (43) as a risk factor for mood disorders such that having a SARS-CoV-2 infection could affect the results of STAI.
Notwithstanding, after analyzing the STAI questionnaire results, neither were any significant differences detected. We observed, however, a tendency for more anxiety in the infected cohort suggesting the sample size was too small to reveal this effect. More work is thus needed to confirm this in a larger study sample.
As far as we know, no study has examined the impacts of coronavirus disease on anxiety. In a recent study (44) conducted in the US general population, an increase in overall anxiety was related to the pandemic's restrictions, especially affecting women. This could perhaps explain the non-significant results obtained in our study, as it seems that rather than the infection itself being the stressor, the home order restrictions imposed could have been a major cause of stress for both cohorts. Effectively, in a recent review (45), several similar factors were identified as stressors including isolation duration, fear of the disease, boredom or frustration, inadequate supplies, and inadequate information.
There is also evidence to suggest (46) that a person with a kidney transplant might not be so emotionally affected by the pandemic due mainly to three factors: experience, knowledge, and traumatic growth. Hence, having lived through their kidney disease, these individuals could have experienced posttraumatic growth or acquired a resilience that helps them adapt to stressful situations.
We should highlight our finding that, depending on the given cohort, age had one effect or another such that when the subject had not experienced SARS-CoV-2 infection, the older the age, the greater the level of anxiety, while older subjects who had gone through the infection showed a lower anxiety level. Studies are needed to identify the possible causes of these differences.
Because of the current pandemic situation and the high level of anxiety detected here in persons with a kidney transplant, there seems to be a need for formal screening at the outpatient nursing unit, so that individualized psychological interventions can be planned to improve the general health of these individuals.
LIMITATIONS
We should mention it was a single-center trial so caution should be taken when generalizing its results. Another issue is its short period designed to minimize memory biases that, nevertheless, limited our sample size. To circumvent this problem, we accessed the universe of individuals who had suffered SARS-CoV-2 infection in our population over the study period.
Our results provide a snapshot of the impact of SARS-CoV-2 infection on the mental health of persons with a kidney transplant. It would be interesting to examine these factors longitudinally, as the pandemic continues, and it could be that we have yet to determine the whole picture of its negative consequences on mental health.
CONCLUSIONS
The findings of this study reveal an affected QoL of individuals with a kidney transplant regardless of whether they have had SARS-CoV-2 infection or not.
In both participant cohorts, anxiety levels were also similarly high.
Over the study period, mortality was low. In contrast, a high rate of case fatalities attributable to the virus was recorded, especially when compared to the rate for the population at large.
Our data analysis revealed that SARS-CoV-2 infection in the population examined was in line with published estimates for the Spanish general population. Global SARS-CoV-2 infection incidences in kidney transplant recipients could not be compared because of the lack of literature data. Indeed, it could be that the data provided here are the first of these characteristics at the national level.
CONFLICT OF INTEREST AND FUNDING SOURCES
The authors declare no conflicts of interest and no funding from any source.
ACKNOWLEDGEMENTS
We are indebted to the Unidad de Investigación del IdISSC, in particular to Dr. Manuel Fuentes-Ferrer, for his invaluable help with analyzing the data obtained.

