











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIn order to diagnose prostate cancer, a prostate bi opsy needs to be performed either under general or local anesthesia.
As with any puncture, bleeding is the most common complication after a prostate biopsy. Hematuria, hema tospermia, and rectal bleeding are commonly self-limited complications and occur in up to 90% of patients1.
We describe the case of a patient who developed a hemoperitoneum after a transperineal prostate biopsy.
Clinical case
A 65-year-old man with a history of prostate cancer diagnosed in 2016 by transurethral resection of the prostate (TURP), with 5% well-differentiated prostate ductal adenocarcinoma, no Gleason score informed, presented to our hospital. He had no further urologic control until 2020 when a rise in the serum prostate-specific antigen (PSA) was diagnosed: 4.49 ng/ml compared to values of 2.11 ng/ml in 2016. Digital rec tal examination showed a 2 × 2 cm prostate with no suspi cious nodules. Magnetic resonance imaging (MRI) informed a 20g prostate anda suspicious lesion reported as Prostate Imaging-Reporting and Data System (PIRADS)2 III in the right mid gland, at the peripheral zone, lateral posterior with no extracapsular extension.
As most prostate tumors are localized in the peripherical zone, which was not biopsied by the previous TURP, a target transperineal fusion biopsy was performed guided by ultra sound (US). Pre-surgical blood tests including coagulogram were normal. There was no associated medical condition recorded. There was no history of aspirin or anticoagulant drugs intake.
Under general anesthesia, 24 cores were taken: Six cores into the target zone and an additional standard biopsy of 18 cores. No immediate postoperative complications were recorded, and the patient was discharged from the hospital hours after the procedure.
Twelve hours later, he reached our emergency service after a head concussion due to orthostatic hypotension. Ad ditionally, he referred increasing diffuse abdominal pain. He had presented hematuriajust in the first micturition after the biopsy, which is expected after this kind of procedure.
A brain computed tomography (CT) scan was performed due to the head concussion, with no abnormal findings. Blood test showed a drop in the hematocrit and hemoglobin values (9% and 3 g/dl points after surgery respectively). Abdominal US showed free intraperitoneal liquid with echogenic material in the bladder dome, suggesting clots (Fig. 1).
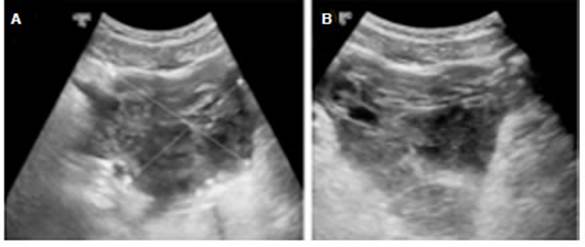
Fig 1 Image A shows US with hematic collection on top of the bladder measured 80 × 89 mm. Image B shows US with hematic collection measured 75 × 50 mm
Consequently, an abdomino-pelvic CT scan showed free intraperitoneal fluid with intermediate density in perihepatic, perisplenic regions, interloop spaces, and along the paracolic gutter (Fig. 2). Additionally, a hematic collection on top of the bladder and in straight relation to the prostate of 104 × 86 mm (intraperitoneal) was observed. No leakage of urine from a bladder or ureters was seen. Active bleeding was excluded.
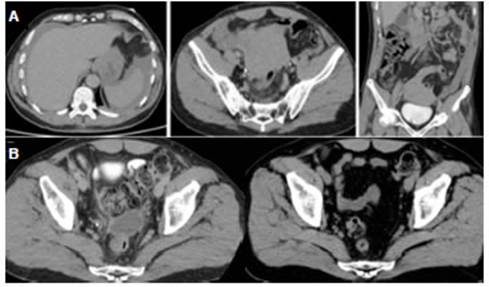
Fig. 2 Image A, CT scan showing free intraperitoneal fluid with intermediate density in perihepatic, perisplenic regions, interloop spaces, and along the paracolic gutter. Hematic collection on top of the bladder and in straight relation to prostate gland of 104× 86 mm (intraperitoneal). Image B, Left side image: CT scan showing 71 mm hematic collection surrounding prostate gland. Right side image: CT showing no collection after 5 months
The patient was admitted to the intensive care unit be cause of persistent hypotension despite fluid restoration. The patient received a single-unit blood transfusion with an increase of 2 points in hematocrit and 0.6 g/dl hemoglobin and presented good response to vasopressors. No further images were performed. Abdominal pain decreased. The patient was discharged from the hospital with stable hematocrit 48 hours after the admission.
One month after the surgery, an abdominal CT scan showed a 71mm hematic collection surrounding the prostate (previously measuring 104 mm) (Fig. 2). The pathological report showed a prostatic adenocarcinoma Gleason score 3+4 in 3 out of 24 cores, just 1 of these was from the tar get zone. Radiotherapy 80 Gy plus androgen deprivation therapy for six months was indicated. The patient did not have sequels and there was no further collection at CT performed for radiotherapy planning, 5 months after the biopsy. (Fig. 2).
Discussion
Some of the most common complications after prostate biopsy are infection and bleeding1,3, usually presenting as haematuria, which is self-limited. These seldom require hospitalization with a readmission rate within 1-4%4,5. Even though there are many publications about exten sive bleedings after the procedure6-9, we have not found previous reports of hemoperitoneum after transperineal prostate biopsy.
Because there was a suspicious area, we took more samples than we usually do in patients with negative RMN. However, we do not consider this as the cause of such bleeding.
CT has a high sensitivity for the detection of even small effusions of blood in the peritoneal cavity10. Spe cific CT signs, such as a sentinel clot or extravasation of intravascular contrast material, may indicate the source of bleeding and help direct management. In addition, the configuration of accumulated blood may help identify the injured organ11.
In most cases of hemoperitoneum, CT obviates in vasive procedures such as exploratory laparotomy and catheter angiography, making conservative therapy a vi able option in patients who are hemodynamically stable12. The angio-CT (with an initial arterial contrast phase, fol lowed by the venous phase) has a similar diagnosis rate as conventional angiography, allowing to differentiate whether bleeding comes from artery or vein13. Although angiography is the best method in cases where a high suspicion of arterial bleeding in the pelvis or extraperito neal organs is considered, its use is limited when there are various bleeding sites or in venous bleeding.
In cases of active bleeding with unstable patients, the election is to perform surgery14. The laparoscopic approach or open exploration is recommended in cases of acute abdo men with an uncertain diagnosis. Moreover, urgent radiologic angioembolization should be considered when possible.
As CT showed no active bleeding and the patient was stable with clinical management, no further procedures were needed.
The authors could not find a clear theory to explain this kind of complication. There are two main questions to be answered. The first is which vessel was damaged during the puncture. Secondly, how could the blood reach the abdominal cavity. Damage during the puncture that involved branches from the inferior vesical artery is one of them since blood from this artery is delivered to the bladder fundus, prostate, and seminal vesicles15. But the reason why the blood passed through the peritoneal layer of the peritoneum to the abdominal cavity remains unexplained. We hypothesize that maybe the previous TURP made some anatomical changes that facilitate the passage to the abdominal cavity.

