











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkKEY POINTS
Current knowledge
• Paget’s disease of bone is a localized benign process characterized by excessive osteoclastic resorption, fol lowed by exaggerated poor bone formation. Its global incidence and neurological and orthopedic complications have decreased in the last 25 years. Updated informa tion regarding the clinical presentation, diagnosis, and management in Latin America is scarce.
Contribution of the article to current knowledge
• Our cohort of PDB patients was mostly asymptom atic with a discreet monostotic presentation and female predominance. These results show a change in PDB epidemiology towards a more indolent presentation, with a lower frequency of orthopedic and neurologic complica tions compared to previous cohorts.
Paget’s Disease of Bone (PDB), described by James Paget as deforming osteitis, is a chronic disease that can affect one or several bones, but never the entire skeleton1. The cause of the disease remains unknown, but currently, the most accepted hypothesis is that it is triggered by a viral infection in individuals genetically pre disposed2. It is a localized benign process characterized by excessive osteoclastic resorption, followed by exag gerated poor bone formation. This process eventually leads to an architectonically altered, painful, deformed and fragile bone3-6.
PDB’s global incidence has decreased in the last 25 years due to the decline in viral infections; its neurologi cal and orthopedic complications have also diminished after the introduction of potent bisphosphonates for its treatment7. In the year 2002, PDB was the second most common metabolic bone disease in the UK, with a preva lence of 6% in ≥ 75 year-old patients8. In most countries of Latin America, the prevalence of PDB is low9-11. However, Brazil and Argentina are the countries presenting the largest cohorts in the region, probably due to the higher prevalence of European immigration9-11. In an osteoporosis center in Brazil, the prevalence of PDB was 0.68%12, which is similar to the epidemiological data reported in Italy and Spain13,14. In 2001, Gómez Acotto and Mautalen described 145 patients with PDB in Argentina, 95% being European descendants11. Unfortunately, updated information regard ing the clinical presentation, diagnosis, and management of patients with PDB in Latin America is scarce.
In our study, the primary objective was to describe the clinical characteristics, diagnostic evaluation, choice of treatment, responses to treatment and clinical evolution in a group of patients with PDB from a specialized center in Argentina. We also aimed to determine the frequency of the diagnosis of PDB in our institution in relation to other bone diseases.
Materials and methods
We assessed all patients attending our institution for bone diseases from June 2012 to December 2019. We reviewed the clinical records and laboratory findings of all the patients diagnosed with PDB3 followed up for more than a year after diagnosis. We gathered these data: reason for consultation, pattern of bone compromise and diagnostic methodology used. Patients with at least one first-degree relative affected by PDB were defined as familial cases. The remaining patients were considered sporadic cases.
We evaluated the response to different treatments. We defined favorable response as levels of total alkaline phos phatase (ALP) and bone phosphatase (BAP) below 50% of the maximum level of the method. Finally, we reported the complications presented by our patients during follow-up.
The relative frequency of Paget’s disease of bone in our population was estimated after analyzing the diagnosis of other phosphorus and calcium metabolism disorders: osteoporosis, primary hyperparathyroidism, Südeck and hypoparathyroidism over the aforementioned period.
The following laboratory parameters were assessed: cal cium [normal values (NV): 8.8-10.5 mg/dl], phosphorus (NV: 2.5-4.5 mg/dl), vitamin D 25 OH (NV: > 30 ng/ml), alka line phosphatase APL (NV: 30-120 IU/L), bone specific ALP (NV: < 21.3 μg/l), parathyroid hormone (PTHi, NV:10-65 pg/ ml), C-terminal cross-linked telopeptide of type I collagen (CTX, NV: women: 556 ± 226 pg/ml, men: 304± 200) and osteocalcin (BGP, NV: 11-43 ng/ml). PTHi, CTX, and BGP values were measured by the Elecsys Roche (Cobas e-411) with a electrochemiluminescence assay (Roche Diagnostics GmbH, Mannheim, Germany). Calcium and phosphorus were measured using Cobas Integra/Cobas c systems (Roche Diagnostics GmbH, Mannheim, Germany). Bone specific ALP and 25-hydroxivitamin D were measured using Liaison XL Assay (Diasorin Inc, Stillwater, MN, USA). ALP was measured by Beckman Coulter AU chemistry analysers, Brea, CA, USA.
Continuous variables with normal distribution were pre sented as mean (standard deviation [SD]); non-normal vari ables were reported as median (range). Categorical data are presented as frequencies and percentages (%). The normal distribution of continuous data was assessed using the Kolmogorov-Smirnov or Shapiro-Wilk test when appropri ate. The comparison of proportions between the groups of monostotic and polyostotic patients was made with the Fisher Exact test. To compare pre and post treatment analytes, the Student’s t test of paired samples was used. Box plots were used to describe the results graphically. Data were analyzed by means of IBM SPSS Statistics 26.0. A value of p<0.05 was considered significant.
The study was reviewed and approved by the research committee of our institution who decided that informed consent was not necessary due to the observational and retrospective design of the study and that it did not represent any risk for the participants. The study was conducted in accordance with the National Law 25.326 of Personal Data Protection, and the principles expressed in the Declaration of Helsinki.
Results
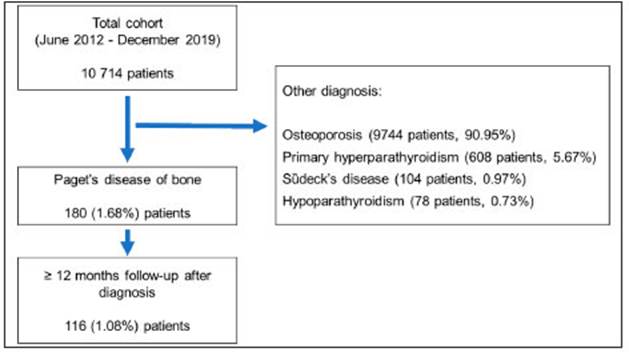
A total of 10 714 patients were assessed, of whom 180 (1.68%) had been diagnosed with PDB. This disease represented the third pathology in terms of frequency after osteoporosis (90.95%) and primary hyperparathyroidism (5.67%). It was more frequent than Südeck’s disease (0.97%) and hypoparathyroidism (0.73%). Of the 180 PDB patients, 116 were followed up for more than a year and were included in the final analysis (Fig. 1). The 59.5% were women. Median age at the time of consultation was 67 (range 39-97) years, 98% were sporadic cases.
The 41% of patients were symptomatic at the time of diagnosis, with the most common symptom being bone pain (83%). Other less common symptoms were patho logic fractures (4.2%), headache (2.1%), radiculopathy (2.1%), secondary osteoarthritis (2.1%), hearing loss (2.1%), hypercalciuria and nephrolithiasis (2.1%). In asymptomatic patients, the diagnosis was based on ac cidental x-ray findings (5.9%) and on persistent elevated ALP levels found in routine laboratory tests in the rest.
The 54.3% of the patients had monostotic disease whereas 45.7% were polyostotic. The affected bones are shown in Table 1, the pelvis being the most reported site. The diagnosis of certainty of PDB was based on both x-rays and bone scintigraphy in (53/116) 46.5%, on bone scintigraphy alone in (31/116) 26.7% and only on x-rays in (29/116) 25%. CT scans were used in (17/116) 14.6% and MRI in (11/116) 9.5%. Both methods were helpful in clarifying anatomic details of the disease, but they were not confirmatory. A bone biopsy was performed in 9 patients, in 7 because they had doubtful monostotic lesions and in two who had a concomitant neoplastic disease, with the purpose of differentiating PDB from metastases.

Table 1 Sites of bone involvement in the monostotic and polyostotic groups in Paget´s disease of bone
Of the 76 patients who required treatment for active disease, 36 (49.3%) received zolendronate 5 mg/year, 14 (19.2%) pamidronate 180-270 mg/year, 10 (13.7%) intravenous ibandronate 12 mg/year and 13 (17.8%) oral bisphophonates (6 were treated with risendronate 150 mg/ month, 5 with ibandronate 150 mg/month and 2 with alen dronate 70 mg/week). There were no differences in the election of treatment between monostotic or polyostotic forms (Table 2).

The percentages of favorable response were 100% for zolendronate, 71.4% for pamidronate, 90% for ibandro nate and 92.3% for oral bisphophonates. Of the 6 patients who did not respond (4 to pamidronate, 1 to ibandronate and 1 to oral bisphonates), 5 received zolendronate with good clinical and biochemical response. The remaining patient refused to receive zolendronate. The percentages of response were not different between monostotic or polyostotic forms (Table 2).
Basal biochemical parameters were evaluated in 76 patients with active disease who required treatment and were compared to measurements made at a median of 6 (range 3-12) months post-treatment (Table 3). ALP, bone specific ALP and CTX decreased significantly after treatment (Fig. 2).
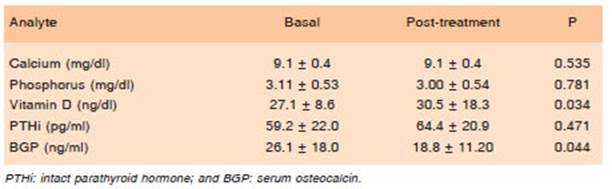
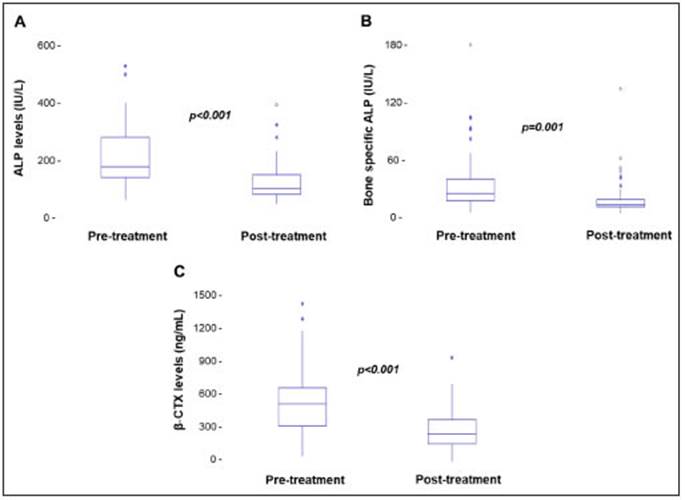
Fig. 2 Boxplots showing a significantly decrease in total and bone specific alkaline phosphatase (ALP) and beta-C-terminal cross-linked telopeptide of type I collagen (β-CTX) serum levels in PDB patients after treatment with bisphosphonates (n = 76). Statistical analysis was performed by Student’s t test for paired samples
The following complications were reported: bone de formities, 2.58%; fractures, 3.44%; nerve root compres sion, 3.44%; arthrosis, 25.8%. Some patients with skull compromise (33.44%) developed hearing deficit.
As regards basal laboratory results, 13 patients (11.2%) had elevated PTHi values with normal vitamin D levels. After receiving bisphophonates, the number of patients with PTHi increased to 15 (12.93%). In the group with elevated PTHi, 5 (4.31%) developed hypercalcemic hyperparathyroidism and a parathyroid adenoma was removed. Eleven patients (9.47%) had nephrolithiasis, the most common metabolic diagnosis being hyperuricusoria and hypercalciuria.
Discussion
Our cohort of PDB patients was mostly asymptomatic, with a discreet predominance of monostotic presentation and female gender. It seems that these results show a change in PDB epidemiology towards a more indolent presenta tion, with a lower frequency of orthopedic and neurologic complications compared to previous cohorts8-10,15-17.
The incidence of Piaget’s disease of bone has de creased significantly in the last 25 years all over the world7, which is probably due to an overall improvement in worldwide public health. Racial differences are known to have an impact on the possibility of developing this benign bone disorder which is particularly frequent among over 50-year-old Caucasians from the United Kingdom, Italy and Spain, whereas it seems to be infrequent among Scandinavians and Asian and Middle East immigrants in European countries15-18. In Argentina, it seems to be a rare condition among American natives and relatively frequent in cities with high rates of European immigration11,19. In our center, it was an infrequent reason for consultation be tween 2012-2019, as only 1.68% of all patients consulted for PDB. This is probably due to two main reasons: this pathology is not so prevalent in our country, and on the other hand, it might reflect the decreasing global trend of its incidence.
The median age in our cohort was 67 years, which coincides with data reported in the literature, where most diagnoses are made as of the fifth decade8-10,16-18. There is a discrepancy, though, with data reported in the world8-10,16-18, as regards the discreet female predominance, for the PDB is classically described as a male-predominant pathol ogy. This is probably a referral bias, as our institution is a referral center for the study and treatment of osteoporosis, a pathology with a clearly higher incidence in women20.
Monostotic, asymptomatic and mild presentations surpassed the frequency of polyostotic, symptomatic and severe disease. This coincides with the world pattern of emergence of a less severe disease, early diagnosis and use of potent bisphosphonates for its treatment7.
As it has been described in all the international series, the affected bones were, in order of frequency, the pelvic, vertebrae, femurs, tibias and skull8-10,16-18. Other bones were less frequently affected such as the ribs and in an ex ceptional case, a kneecap, as part of polyostotic disease.
It is worth noting the prevalence of asymptomatic cases, which in most cases were diagnosed as a result of a persistently raised alkaline phosphatase level found in routine laboratory tests. In a Dutch population study of 4406 people, Paget´s disease was radiographically confirmed in 20.5% of subjects who had raised alkaline phosphatase, whereas only 2.3 % of PDB patients had normal biochemical values21. This proves the importance of this isolated laboratory finding in the search for Paget’s disease among men and women over 50 years of age.
As regards diagnostic imaging, plain x-rays and bone scintigraphies were the most useful methods, both in dependently or combined. The international guidelines recommend making a full body bone scan to detect all the active sites of the disease and full skeleton x-rays so as not to omit inactive sites or those in final stages of fibrosis3-6. Our team prefers to start the imaging diagnosis by performing a bone scan and afterwards an x-ray of all the sites where Paget´s disease is suspected, so as to reduce the patient´s exposure to radiation. We only needed to use more sophisticated imaging methods to evaluate complications of this disease and we performed bone biopsy in cases of diagnostic doubt in monostotic lesions or in patients with concomitant malignant diseases as suggested by international guidelines5.
In the laboratory, the levels of ALP, bone specific ALP and CTX decreased significantly after treatment. BGP, a marker of bone turnover which is very useful in other pathologies, was not helpful in PDB. Our findings coincide with those reported in the literature22-24. Apparently, deter mination of urinary NYX is the test that best correlates with the degree of activity of the disease22,23. It is evaluated by bone scan and it is considered the best method, but this test is not frequent in our country.
Aminobisphophonates are the first line of treatment for PBD3-5,25-27 and the introduction of zolendronate has allowed long-term remissions of the disease25-28. In the analyzed time period, 2012- 2019, we changed progres sively from pamindronate to zolendronate, achieving very good results. A distinctive feature of our population is that we achieved good results with less potent drugs such as intravenous ibandronate and risendronate and oral alendronate, in doses and schemes similar to those for treating osteoporosis.
The orthopedic and neurologic complications of our patients were fewer than those reported in the historical series8-10,16-18, although ours is a cut-off research and not a real follow-up study and we covered a period of just eight years. Conversely, metabolic complications such as hyper calcemia due to parathyroid adenoma and nephrolithiasis associated with hypercalciuria and hyperuricosuria were as frequent as those reported in the Mayo Clinic series17 that evaluated complications in a data base that covered patients with diagnosis of PDB between 1950 and 2008. We have already reported our experience with the associa tion between hyperparathyroidism and PDB29.
Our study has several limitations: it is an observational, retrospective study and reflects a single-institute experi ence in the management of the disease. This work does not allow us to endorse changes in the epidemiology of PBD because our computerized registry of diagnoses began in 2012 and we were unable to compare our data with what happened in previous years. On the other hand, our institution is a referral center for the diagnosis and treatment of PBD and it could be necessary to carry out a multicenter study of the entire country to support a change in the epidemiology of this disease.
As a conclusion, we can point out that PBD was not a frequent cause of consultation in our center. Mild, oligo symptomatic and monostotic forms were predominant, with low frequency of orthopedic and neurologic complica tions. In the future, this change in the epidemiology of PDB would probably allow a decrease in the doses of bispho phonates historically recommended for these patients.

