











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
The prevalence of respiratory complications after COVID-19 pneumonia is currently unknown, but the data obtained from previous coronavirus outbreaks may provide important information1.
Some reports state that between 20% and 60% of survivors of the global SARS (severe acute respi ratory syndrome) outbreak caused by SARS-CoV (SARS-associated coronavirus) and MERS-CoV (Middle East respiratory syndrome coronavirus) experienced some persistent physiological dete rioration and pulmonary images compatible with fibrosis1.
The preliminary evidence supports the hypoth esis that some survivors could develop long-term respiratory sequelae. Pulmonary fibrotic anoma lies have been detected three weeks after the onset of symptoms, regardless of the degree of severity of the disease (mild, moderate or severe)2.
We present three patients with moderate to severe pneumonia, who required oxygen, antibiot ics and corticosteroids but never needed invasive mechanical respiratory assistance (MRA). Follow-up computed tomography scans between 30 and 60 days after discharge showed images with inter stitial infiltrates compatible with post-COVID-19 pneumonia pulmonary fibrosis.
CLINICAL CASES
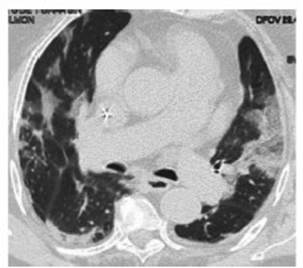
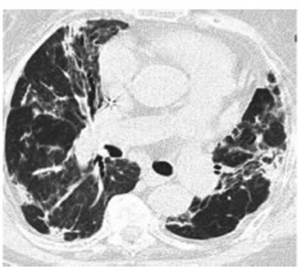
Case 1: 84-year-old female patient, with history of light smoking (5 packages per year), obesity, arterial hyperten sion (AHT), chronic renal failure and coronary disease. The patient was hospitalized in the ward due to moderate COVID-19 pneumonia (according to the severity criteria of the 2007 ATS/IDSA [American Thoracic Society/Infectious Diseases Society of America] Guidelines) (3) for 34 days; chest CT done on admission (Figure 1). She received anti biotic treatment (ampicillin/sulbactam [AMS], 1.5 g every 6 h for 10 days, and clarithromycin, 500 mg every 12 h for 10 days), oxygen therapy (with nasal cannula, between 3 L/min and 4 L/min for 3 days), and corticosteroid therapy (dexa methasone, 8 mg per day for 10 days). Follow-up CT scan done two months after the onset of symptoms (Figure 2).
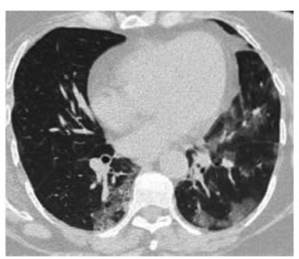
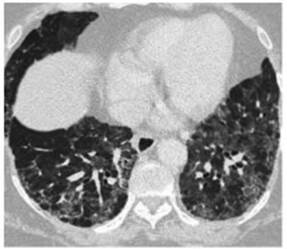
Case 2: 58-year-old female patient with history of obesity, a professional nurse. Hospitalized due to moderate to severe COVID-19 pneumonia (according to the severity criteria of the 2007 ATS/IDSA Guidelines)3 for 18 days, requiring oxygen therapy (with nasal cannula at 6 L/min for 6 days) and non-invasive ventilation (NIV), (pressure support ventilation [PSV], inspiratory positive airway pressure [IPAP]: 10, expiratory positive airway pressure [EPAP]: 5 for 2 days) in a closed unit; she also received 2 units of convalescent plasma, antibiotic treatment (AMS, 1.5 g every 6 h for 10 days and clarithromycin, 500 mg every 12 h for 10 days) and corticosteroid therapy (dexamethasone, 8 mg per day for 10 days). Chest CT done on admission (Figure 3). Follow-up CT scan done 2 months after discharge due to persistent dyspnea FC II/III. (Figure 4).
Case 3: 63-year-old male patient with history of smok ing (32 packages per year), diabetic. Hospitalized in the ward due to moderate COVID-19 pneumonia (according to the severity criteria of the 2007 ATS/IDSA Guidelines) (3) for 17 days. While hospitalized, the patient required oxygen therapy (with nasal cannula at 3 L/min for 2 days), corticosteroid therapy (dexamethasone, 8 mg per day for 10 days) and antibiotic treatment (AMS, 1.5 g every 6 h for 7 days and clarithromycin, 500 mg every 12 h for 7 days). Chest CT done on admission (Figure 5). 20 days after dis charge, the patient attended the on-call service with dys pnea, functional class III/IV. CT was done with pulmonary thromboembolism (PTE) protocol, without positive result, and progression of septal thickening to subpleural predomi nance and honeycombing were evidenced in parenchymal window (not present in the previous study). Symptoms are interpreted as secondary to the sequelae of previous pneu monia; no new supplementary tests were done (Figure 6).


DISCUSSION
It’s a well-known fact that many patients suffering from acute respiratory distress syndrome (ARDS) experience deterioration of their quality of life, years after the disease, despite the breakthrough in clinical care related to the pulmonary protection strategies of mechanical ventilation.
A percentage of ARDS survivors develop a fibroproliferative response characterized by the accumulation of fibroblasts and deposit of collagen and other elements of the extracellular matrix in the lung.
The development of severe fibroproliferative lung disease has been associated with bad prog nosis and high mortality rates4.
Four stages of COVID-19 at chest CT have been described: early stage (0 to 5 days after the onset of symptoms), characterized by normal findings or mainly ground glass opacities; progressive stage (5-8 days after the onset of symptoms), may show increase in ground glass opacities and crazy paving; peak stage (9 to 13 days after the onset of symptoms), characterized by progressive consolidation; and late stage (≥ 14 days after the onset of symptoms), characterized by a gradual decrease in consolidation and ground glass opaci ties, whereas signs of pulmonary fibrosis can start manifesting (including interstitial parenchymal bands, lung architectural distortion and traction bronchiectasis)5.
Patients referred to chest CT must do it with out contrast, unless CT pulmonary angiogram is required to detect pulmonary thromboembolism (PTE)5.
If a follow-up CT scan is to be done, we suggest the use of a low radiation dose protocol in order to minimize the radiation load5.
A cohort study of COVID-19 patients, with follow-up done six months after discharge, which, as mentioned by the authors, is the larg est study with the longest follow-up duration of discharged patients, showed that the evaluation of the lung function in a considerable propor tion (22%-56% in different degrees of severity) of participants showed certain deterioration of the diffusing capacity of the lungs for carbon monoxide (DLCO), six months after the onset of symptoms. This was consistent with the findings that the abnormal patterns most frequently found in the chest CT were interstitial pulmonary infiltrates (ground glass infiltrates and septal thickening).
The respiratory viral infection could poten tially induce a different fibroblast activation in the convalescence phase. We found that, the more severe the disease in the acute phase, the more important the alteration in the DLCO and tomographic pattern.
The results of this study didn’t suggest that corticosteroids can accelerate pulmonary lesion recovery in the evaluation of the lung function and chest images, even though the evidence has shown the benefits of this treatment for patients with severe COVID-19 in the acute phase6.
In agreement with these results, another study was published with the follow-up of patients who required hospitalization in the intensive care unit (ICU) and were evaluated three months after hospital discharge. The follow-up included symptoms and quality of life, anxiety and depression questionnaires, lung function tests, 6-minute walk test (6MWT) and chest CT. We found that there is a relationship between age and days of MRA and tomographic findings. The main patterns that were found were ground glass infiltrates (59.6%), septal thickening (80.7%) and bronchiectasis (71.9%). The rate of reticular and fibrotic lesions was 49.1%, even higher than the rate of survivors of other viral types of pneumonia, including SARS, H1N1 and H7N97.
Recent studies have also shown that patients with COVID-19 are more frequently hospitalized, have longer hospital stays and higher risk of de veloping SDRA, in comparison with patients with other acute respiratory diseases7,8.
In relation to the large number of patients with pneumonia caused by SARS-CoV2 and the possible risk of pulmonary sequelae, it is impor tant to do a follow-up in order to detect possible complications.
To do so, various societies of respiratory medicine have published some recommenda tions for the clinical and radiological follow-up that suggest control of pulmonary images and lung function tests mainly according to the se verity of the condition and the presence at the moment of clinical symptoms, at a reasonable interval1,9,10.
The purpose of this series is to show examples of possible sequelae in patients who have suffered COVID-19 pneumonia.

