











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
One of the biggest challenges in the aging population, which is also observed in Brazil, is oral health. Overall, most elderly people present poor oral health, as shown by higher rates of periodontitis and dental caries1,2. These conditions are chronic, irreversible and present a cumulative effect, often leading to tooth extraction as the only treatment option3.
The literature reports that tooth loss may negatively impact quality of life of the elderly4. Its extension and severity over life may cause major deleterious effects on functional, esthetic, nutritional, psychological and social aspects5. The higher prevalence of oral diseases may affect overall health, impairing the aging process per se. This condition also has major economic impact, as oral rehabilitation is very expensive6.
Although mean tooth loss and prevalence of edentulism have been decreasing over the years, they are still major problems in several underdeveloped countries, especially among the elderly7,8. Tooth loss is considered severe when the individual has less than nine permanent teeth9, and this condition is reported as being highly prevalent in most studies conducted with Brazilian elderly people during recent decades2,10.
Tooth loss may also be considered as a marker of social inequalities, as in developed countries, the rate of tooth loss did not decrease among less economically privileged individuals as much as it did in other socioeconomic classes11. This scenario may be more alarming in undeveloped countries, such as Brazil, where social and educational inequalities are more evident. Tooth loss is also a true outcome in Dentistry and is probably the best proxy of overall oral health. The aim of the present study was to investigate severe tooth loss and its associated factors among the elderly in a city in southern Brazil. The study hypothesis is that demography, socioeconomics, access to care and health habits are associated with severe tooth loss.
MATERIAL AND METHODS
Study design, location and ethical aspects
This cross-sectional study interviewed and examined elderly persons aged 65 to 74 years living in the urban area of Cruz Alta, a city located in the State of Rio Grande do Sul, Brazil. According to the latest census, city population was 62,82112, with more than 95% living in the urban area. Of these, 3,730 are in the 65- to 74-year age stratum, 42% are male and 58% are female. In 2010, the Gini Index was 0.541913.
The present study was reviewed and approved by the Institutional Review Board of the University of Passo Fundo (UPF) under protocol #1.531.862. All participants signed informed consent before their inclusion in the study.
Sample size calculation and sampling strategy
The formula used for sample size calculation was: sample size = standard normal variate2 x outcome prevalence x (1 - outcome prevalence)/absolute error2. We assumed a type error of 5% (standard normal variate of 1.96) and an absolute error of 0.1%. The estimated sample size calculation used the prevalence of tooth loss in the elderly, as previously reported, as 94.72%14. Therefore, the total number of individuals considered necessary was 205. Due to the expected attrition rate, we added 20% to the final sample, estimating a total 246.
A probabilistic per conglomerate sampling was performed by visiting 300 households. Further details of the sampling strategy may be found elsewhere15. Briefly, the study area consists of 68 neighborhoods and districts, of which 17 (25%) were randomly selected, according to the proportion of elderly people in each area. The blocks and corners were also randomly selected. After the first interview, the visits continued in clockwise direction until sufficient individuals in the sector were included. If necessary, new blocks were selected until the necessary number of households had been visited.
Inclusion and exclusion criteria
Only home-dwelling elderly persons aged 65 to 74 years, from the selected households were included. Elderly persons with physical, medical and mental conditions that enabled this study to be conducted were included. In order to be included, participants also needed to understand the questions in the questionnaire and allow examinations. When there was more than one elderly person who met the inclusion criteria in one household, they were all were invited to participate. Assisted living facilities, commercial living facilities, visitors, and uninhabited households were excluded. A household was excluded only after two unsuccessful visits.
Clinical examination and interview
A structured questionnaire was applied, which included the following variables: demographic data, socioeconomic condition, marital status, oral hygiene habits, behavioral, and health history. All questions were taken from the block of questions of the PCA Tool-SB Brasil, adult version, validated in Brazil16. Oral examination was performed by counting teeth and assessing use of and need for dental prosthesis.
Oral examination was performed according to the World Health Organization recommendations17. Oral examination was performed after the interview, using a wooden spatula, without artificial illumination or dental mirror. All teeth were considered, except for the third molars. Teeth that could be somehow rehabilitated were considered in the count. Teeth or roots that would not possible to be retain in the oral cavity were considered absent.
Participants were interviewed and examined between July and August 2016 by two teams of researchers. Each team consisted of an interviewer and an oral health examiner. They were all trained by the study coordinator in order to standardize fieldwork. The training consisted of theoretical lectures about the study, discussion of each question in the questionnaire, and explanation of how the oral examination should be performed. Prior to the beginning of the study, two examiners were calibrated with elderly persons who sought treatment at the School of Dentistry of the University of Passo Fundo. The examinations were performed twice, with a two-day interval. For intrarater reliability, the kappa coefficient was 1.00 for need for dental prosthesis and 0.85 for tooth count. Inter-rater reliability had a minimum kappa coefficient of 0.70 for all the previously reported variables.
Statistical analyses
Severe tooth loss was defined as the outcome of the present study. It was not possible to perform a linear regression because tooth loss presented a nonsymmetrical distribution (Shapiro-Wilk test showed a p-value <0.001). We used severe tooth loss to dichotomize the sample. Two groups were created, one with individuals with severe tooth loss (0 to 8 remaining teeth) and another with individuals without severe tooth loss (>9 remaining teeth). The independent variables were: age, sex, ethnicity/skin color, level of education, marital status, retirement, oral hygiene habits, use and need of dental prosthesis, access to dental care in the past 12 months, smoking and alcohol exposures, general health problems, and use of medication.
Median age in this sample was 70, so we categorized the sample in two groups: one for age <70 years and another for age >70 years. Ethnicity/skin color was dichotomized into white or non-white. The nonwhite group included participants who reported they were black, yellow, brown or indigenous. Level of education was categorized into low for those that had up to complete elementary level of education, including the illiterate; medium, for those with incomplete or complete high school; and high for those with at least incomplete higher education. Health problems were categorized into two groups, one with participants who reported having at least one health problem, and another with participants who did not know or did not report any health problems. Similarly, the use of medications was also dichotomized into participants who did not use any medication and participants who used at least one medication per day. Toothbrushing frequency was categorized in two groups: <3 times/day or >3 times/day.
All analyses were performed in the software SPSS, version 21.0 (SPSS, version 21.0, IBM Corp., Armonk, NY, USA). Associations between the dependent and independent variables were tested by chi-square of Mann-Whitney tests, and are presented by frequency distribution. Univariate and multivariate analyses were performed using Poisson regression with robust variance. The variables included multivariate model were those that presented a p-value <0.25 in the univariate analysis. A combination of p-value <0.05 and modification of effect analyses determined the maintenance of these variables in the final multivariate model. Multicollinearity analyses were performed among the independent variables, and none was observed. The cutoff point for multi-collinearity was determined as variance inflation factor <5 and tolerance >0.2.
RESULTS
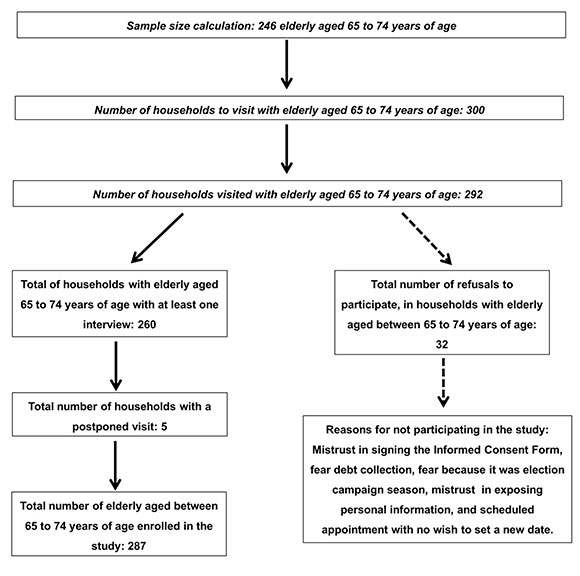
A total 287 elderly persons were interviewed and examined. This number provided the minimum required for the sample to be representative. The response rate was 89.04%, as shown in Fig. 1. Mean age was 69.30 (standard deviation - SD - ±3.52); 102 participants (35.5%) were male and 185 (64.5%) female. Regarding ethnicity/skin color and level of education, 196 (68.3%) were white and 190 (62.6%) had low level of education. Approximately 40% of the participants were single, divorced or widowed, and 76.3% were retired. History of smoking exposure was detected in 42%. Mean (±SD) tooth loss was 19.69(±8.21), and 86 (29.9%) of the participants were edentulous. Prevalence of at least one missing tooth was 98.3% (n=282), and prevalence of severe tooth loss was 60.3% (n=173).
Age (p=0.007), sex (p<0.001), level of education (p<0.001), marital status (p= 0.002), alcohol exposure (p=0.011), and access to dental care (p<0.001) were significantly associated with severe tooth loss (Table 1). Ethnicity (p=0.766) and smoking exposure (p=0.936) were not associated with severe tooth loss.
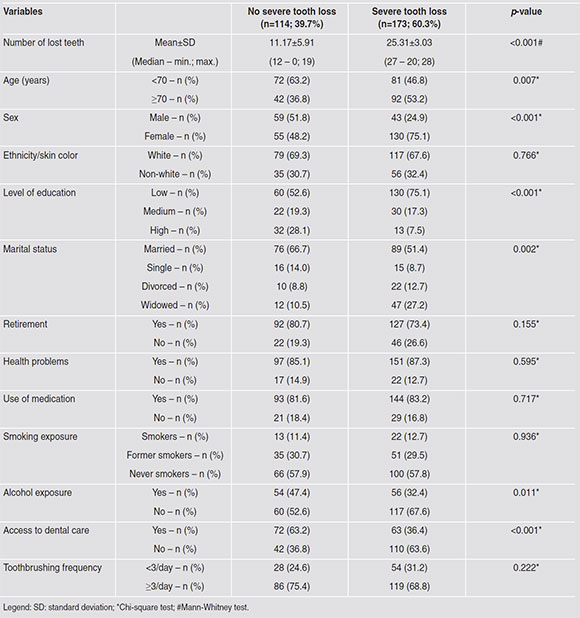
Table 1 Association of demographic, economical and behavioral variables with severe tooth loss, Cruz Alta, Rio Grande do Sul, Brazil, 2016.
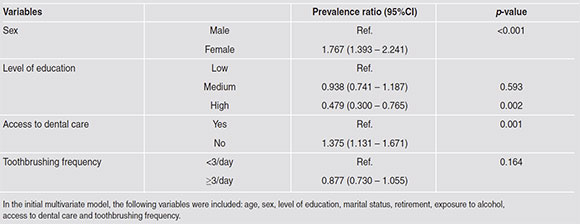
Table 2 shows the univariate analyses of the association between severe tooth loss and independent variables. The following variables were significantly associated with severe tooth loss: age, sex, level of education, marital status, alcohol exposure, and access to dental care. The prevalence ratio (PR) for severe tooth loss was 29.7% higher in participants aged >70 years than in participants aged <70 years (p=0.007); 66.7% higher in females than in males (p<0.001); lower in participants with higher level of education than in those with lower level of education (PR 0.422 - 95% CI: 0.264 - 0.675); and higher among widowed than among married participants (PR; 95% CI: 1.477; 1.220 - 1.788). Participants who were not exposed to alcohol presented 29.8% higher PR of severe tooth loss than participants who drank regularly. Participants who had not visited a dentist in the past 12 month presented 55% higher PR of severe tooth loss (p<0.001) than those who had access to dental care. In the initial multivariate model, the following variables were included: age, sex, level of education, marital status, retirement, exposure to alcohol, toothbrushing frequency, and access to dental care. In the final multivariate model, sex, level of education, and access to dental care remained associated with tooth loss (Table 3). PR for severe tooth loss was 76.7% higher in females than males (p<0.001); lower in participants with high level of education than in participants with low level of education (PR; 95% CI: 0.479; 0.300 - 0.765), and 37.5% higher in participants who had not visited the dentist during the past 12 months (p<0.001). However, toothbrushing frequency did not show statistically significant association with severe tooth loss (p=0.164).
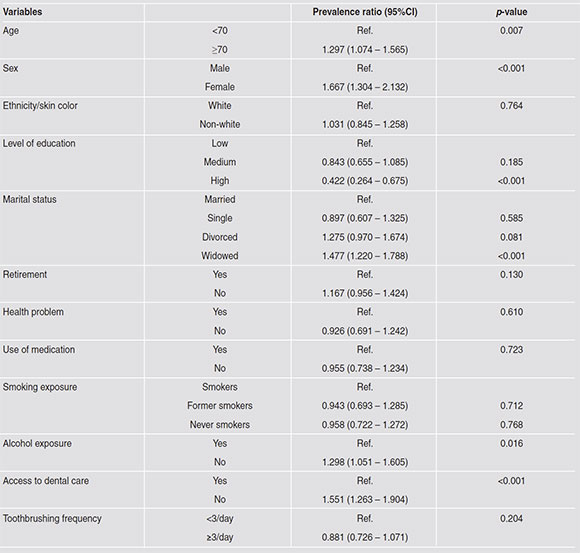
Table 2 Univariate analysis of the association between independent variables and severe tooth loss, Cruz Alta, Rio Grande do Sul, Brazil, 2016.
DISCUSSION
The aim of the present study was to evaluate severe tooth loss and associated factors among the elderly in a city in southern Brazil. Prevalence of tooth loss and severe tooth loss were very high (98.3% and 60.3%, respectively). Mean tooth loss was 19.69 (±8.21), and severe tooth loss was associated with sex, level of education, and access to dental care. Analysis of tooth mortality is very important because it reflects the efficacy of oral care in a population18. In addition, it should be kept in mind that within the oral health field, tooth loss is the most important outcome, i.e. preventive and therapeutic approaches should ultimately aim to maintain functional teeth. Therefore, in this study, tooth loss is considered a true outcome and not a surrogate as it is in most studies in Dentistry19. The literature also shows that, among the elderly, oral health-related quality of life decreases in those that experience at least one tooth extraction within a period of six years20. These results may provide useful information for planning public health policies, including allocation of financial resources for oral rehabilitation of the elderly population.
The high mean tooth loss found in the present study was also reported in other home-based studies conducted in southern Brazil. One study with a representative sample of the metropolitan region of Porto Alegre, Rio Grande do Sul, reported mean tooth loss of 20.210. Another two studies conducted in different cities in Brazil showed mean tooth loss ranging from 18.7 to 19.21 in the elderly2,21. National mean tooth loss for the aged is 25.29, according to the latest national oral health survey22.
These results suggest that the oral health of the elderly has not improved as expected over the years. Similar high severity of tooth loss is also widespread in other parts of the world, including developed countries7.
In the present study, female sex was associated with higher PR of severe tooth loss. This result is consistent with a previous report of higher mean tooth loss among elderly females than among elderly males4. Based on these results, it is important to highlight that tooth loss may reflect not only the burden of oral diseases, but also the attitudes of the patients and their dentists, the availability of dental services, and prevailing philosophies during oral treatment1. In fact, women have been found to be more careful about their oral health and also seek more health services than men do,23 and are consequently more exposed to different treatment options, which may include more tooth extractions. In the present study, tooth loss was analyzed including both extracted teeth and teeth whose condition would not allow rehabilitation. Therefore, the question may arise as to whether females are more exposed to overtreatment in terms of extractions.
Similarly, low level of education was associated with higher tooth loss, which has already been reported in the literature, regardless of the socioeconomic characteristics of the country10,24. The level of education may be the most important factor associated with health problems, and it has been used as a proxy of socioeconomic status, including income3. The literature shows that higher level of education is associated with better health conditions and greater longevity25. According to the latest national census, the majority of older Brazilians have a lower level of education12, which was also observed in the presented study. We found that 190 of the participants (66.2%) had up to complete elementary level of education, including the illiterate. It may thus be hypothesized that the lower level of education partially explains the results detected in the present study.
The poor oral health condition observed in the majority of the participants, mainly reflected by high tooth loss, represents the cumulative experience of dental caries and periodontitis, among several other oral diseases26. All those conditions are directly related to the poor health habits of the elderly. The higher frequency of toothbrushing is associated with lower chances of having periodontitis27 and dental caries28, which may impact directly in tooth survival. However, another study showed that the impact of toothbrushing frequency may be small29, while the quality of the brushing technique may be more important. This may explain why the present study did not detect a significant association between toothbrushing frequency and severe tooth loss. Access to oral health information, promotion of preventive aspects of oral health, and oral rehabilitation should be a priority in this age group. The lack of access to dental care during the past 12 months was associated with higher severe tooth loss in this population. It is important to consider that several aspects may be related to the absence of regular visits to the dentist. The cost of oral treatment, fear, and lack of availability are the most frequently cited problems among irregular users of dental services30. Strategies to overcome these problems are of the utmost importance in order to increase the regularity with which the elderly receive dental services.
One of the strengths of this study is that a representative sample of the elderly population in Cruz Alta, Brazil was achieved. When compared to the latest census in the city, the present study included similar proportions of sex, skin color and level of education. Another strength was that the examiners were trained and calibrated in order to ensure reproducibility of the data. However, the study also had some limitations. The cross-sectional design does not allow temporal associations between tooth loss and the independent variables. We did not analyze the reasons for tooth loss. Additionally, we did not perform a linear regression in our analysis, as the distribution of tooth loss in the sample was asymmetrical. Nevertheless, the study design enables data generalization and comparison to other home-based representative studies.
The main outcome of the present study was severe tooth loss. This enables an analytical approach in which different patterns of tooth loss can be compared by trying to assess what the associated factors are. Clearly, the selected cutoff point is high (9 remaining teeth), but it is consistent with previous studies reported in the literature2,9. It should be highlighted that the participants still present a high experience of oral diseases, since the preventive strategies that are used currently did not cover them when they were younger. This distribution is in line with what has been observed in several places31.
The continuous evaluation of tooth loss is very important in order to verify the effectivity of public oral health-related policies, especially among the elderly population. The present study demonstrated that severe tooth loss is very high among the elderly, and found that severe tooth loss is associated with the female sex, low level of education, and lack of access to dental care.

