











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
A consequence of advancing age is the presence of alterations in the masticatory system which involve maxillary, mandible, temporomandibular joint (TMJ) and musculature. Within the latter, the masseter muscle determines the vertical dimension of occlusion (VDO) stabilization. Thus, any degradation involving those structures derives in a functional decompensation 1-3 .
It is currently known that TMJ alterations are not the only cause of occlusion disorders. Temporo mandibular disorders (TMD) related to changes in vertical dimensions with modified functioning of surrounding muscles generate a posterior position in the condyle that can be established using cone-beam computed tomography (CBCT) 4-7 . Some of these alterations are caused by alveolar ridge resorption and changes in biting forces that modify condyle positions inside the articular fossa 8 . Those changes are related to increased mechanical tooth surface wear and may progress to pathological tooth wear (PTW) because of parafunctional mandibular movements which modify masticatory muscle tone, and generate facial pain and aesthetic and phonetic disorders 8-14 .
These alterations plus missing teeth lead to decreased or increased VDO, which is visualized by changes in the distance between the nasal spine (Subnasale, “Sn”) and the most anterior inferior point of the chin (Soft Tissue Menton, “Me”). When the mandible is in physiologic rest position with non-contacting teeth, it is called rest vertical dimension (RVD), which differs from VDO 15-17 .
Many methods have been suggested over the past decades to establish VDO: swallowing, phonetic, rest position, maximum closing force, pre-extraction records, Willis, Landa, McGee, Hayakawa, comfort, cephalometric, anthropometric and Knebelman’s craniometric method, but none of them can register VDO objectively. Original specifications suggest that Knebelman’s method should be applied in normal craniofacial development (mesoprosopic). Later studies found a correlation with leptoprosopic type because of racial characteristics, but they emphasize that there is no applicability for euryprosopic 18-28 . Ricketts defined facial biotype as the morphologic and functional characteristics of the face, reason why, facial biotype is used for treatment plans which depends on the maxillary facial growth pattern 29 where biting force, has been shown to be related to final dental arch form 30 .
This study evaluated the VDO determinations obtained by anthropometric and Knebelman’s craniometric methods.
MATERIALS AND METHODS
A cross-sectional study was performed with 200 adults, selected from patients attending Catholic University of Cuenca dental clinics located in Azogues, Ecuador. Each participant completed an informed consent form. Bioethical and technical aspects of the project were approved by the Catholic University of Cuenca - Azogues authorities under code 00001CIABEOSA.
Demographics (age, sex) and clinical data (edentulism type and facial biotype) were recorded. Trained, calibrated (Kappa= 0.8) clinicians used both the anthropometric method and Knebelman’s craniometric method to determine VDO in all participants. The procedure was conducted under natural light. Patients sat with a straight back.
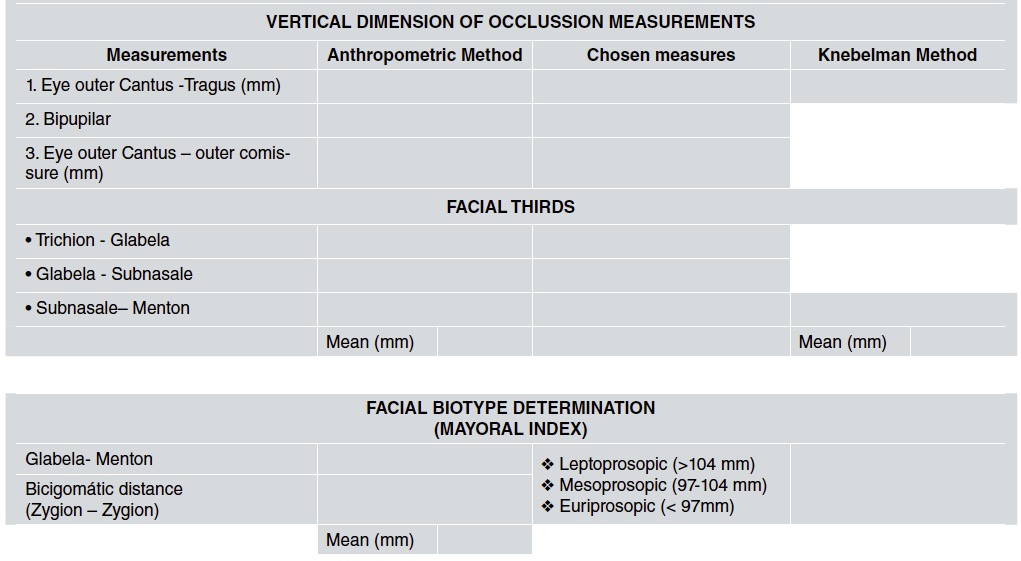
Frankfort plane was established parallel to the floor, occluding for partially dentate patients and reaching rest position for edentulous patients. Once these positions were obtained, anthropometric points were marked using an eye pencil. Facial index was determined using the Mayoral index that uses soft tissues related landmark points (ophryon-menton/zygion-zygion) to register measurements in millimeters. This enabled the distribution of facial types within the sample to be established.
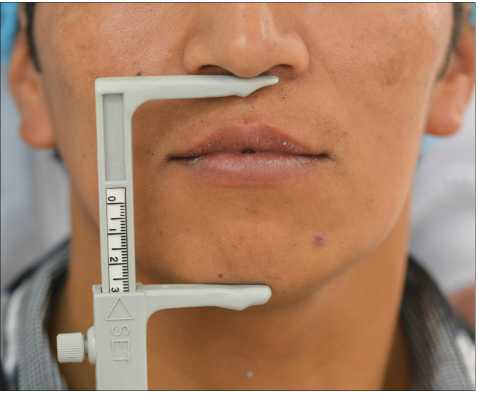
The anthropometric method was applied using a vernier caliper to determine the planes mentioned in Table 1. The measurements were compared to the height of the lower facial third. A ± 2 mm error range between measures was set to define whether vertical dimension was maintained, diminished or increased (Figs. 1 and 2).


Fig. 2 Anthropometric method application (Eye outer Canthus-Outer commissure measurement delimitation)
Knebelman’s Craniometric method was applied using a Knebelman’s craniometer, which only considers two measurements, called “READ”, from external auditory canal to the lateral corner of the bony orbit and “SET” from Sn (subnasal) to the most anterior undersurface of mandible. Both readings are correlated and contribute to the final result (Figs. 3 and 4).

A template was designed on which to record the measurements, allowing selection of measurements not to be considered for the anthropometric method (Table 1).
Statistical analysis was performed by obtaining averages and standard deviation, and differences between the methods were analyzed using the t-test for paired data. Significance level was established at P<0.05.
RESULTS
Tables 2 and 3 show distribution of sex and age, respectively, and tables 4 and 5 show distribution of edentulism type and facial biotype, respectively. The application of the t-test for paired data showed a significant difference (p<0.001) between the two methods (Table 6).
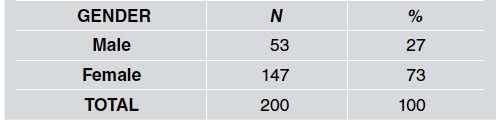

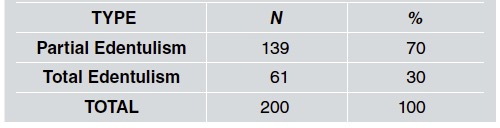
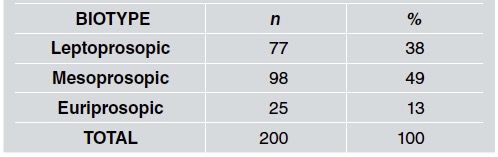

Table 6 T test between anthropometric method and Knebelman’s craniometrie method applied in treated patients.
When facial type is considered (Table 7) the difference between methods was not statistically significant in leptoprosopic patients, though it was significant in the other two groups.

DISCUSSION
Losing natural dentition can lead to alterations in the height of the lower facial third due to increased bite force, so reestablishing VDO improves quality of life by enabling the patient to recover the ability to produce certain movements without any limitation. It is thus important for dentists to obtain precise measurements for an adequate VDO. Ayoub28 reports that interpupillary distance can be used as a VDO determination factor in males. Alhajj, et al29 report that measurements from the outer canthus of the eye to the oral commissure are more reliable for VDO prediction for edentulous patients. According to Bajunaid et al. 30 , facial landmarks mentioned by Misch (about 12 measurements with a difference range between 1-2 mm) are used to determine VDO in edentulous patients reliably and objectively. Distances between left eye-ear and left angle of the eye to angle of mouth showed accuracy in determining VDO for complete denture wearers, as is also mentioned by Majeed et al31 . The Constantiniuc 32 comparison between phonetic, rest position and anthropometric methods to establish VDO did not show relevant differences between final measurements, which suggests that these methods could be applied to help determine VDO in edentulous patients. However, according to Batra 33 , there is no validation for any method proposed to measure VDO. The use of bone points by cephalometric analysis leads to increased accuracy in measurements because there is no facial or positional manipulation determining freeway space, but a functional method must also be used to improve measurements provided by lateral RX in edentulous patients. Ousehal and Sierpinska 34 , 35 report that cephalometric studies could lead to an adequate initial VDO, referring to Knebelman’s craniometer as an adequate way to determine initial VDO that could be complemented with cephalometric studies. One of the most frequently analyzed concerns is considered by Behrensdorf 36 , who says that age and time using dentures affect VDO reestablishment and mandibular movements. According to these conclusions, Fukushima 37 evaluated methods based on condyle position and showed their unreliability due to the effect of muscle action on it. Watarai 38 states that physiologic mandibular rest position could be modified by head or body postures, mental state, muscles and TMJ, emphasizing the difficulties in establishing an accurate position.
On the other hand, Miran 39 claims that the applicability of a specific method to determine VDO depends on accuracy, adaptability, equipment and cost. However, Mahboub40 states that differences in their application using stone casts, pre-extraction records or cephalograms help in the determination of VDO but are not reliable by themselves.
In addition, some studies showed compatibility with the results obtained in the current study. Talavera 18 compared Willis and McGee methods (using craniometrical measures such as Knebelman’s).
Alhajj 29 using a method that involves a finger length shaft, obtained mean measurements that are within the range of values recorded in our study. This information suggests the reliability of the method in different scenarios.
After studying and recording facial biotype and VDO, our results showed a small difference between mean measurements obtained with the two methods under study. Knebelman’s craniometric method seems to be more reliable during the VDO determination process since its variability is lower. It is also easier to apply and reduces diagnosis time. One of its possible disadvantages may be the cost of the instrument. This is the first local study to record VDO and facial biotype, so it could be used as a baseline for further studies.

