











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
INTRODUCTION
The goal of endodontic therapy is to disinfect and obtúrate the root canal system. One of the challenges is the internal morphology and the many anatomical variations of the different tooth groups 1 .
For a long time, one of the main methods for assessing internal anatomy involved clearing, staining and making serial cross-sections of extracted teeth 2 . Now, internal anatomy can be studied using microcomputed tomography (Micro-CT), which is considered the gold standard for this purpose. However, all these techniques are feasible only in ex vivo experiments using extracted teeth 3 . Considering the anatomical aspects among dental types, one study found that root canals in first mandibular incisors were Vertucci type I (50%), II (62%) and III (28%) 4 , and another study found that root canals in lateral mandibular incisors were type I (30.2%) and III (18.9%) 5 . Mandibular first premolars are single-rooted teeth, well known for their anatomical variations, which can pose a challenge for endodontic treatment. Data from over 6,700 mandibular first premolars revealed that single canals were found in 75.8%, and two or more canals in 24.2% of the examined teeth 6 . A single apical foramen was found in 78.9% of the specimens evaluated, while 21.1% had two or more apical foramina 7 .
Mandibular molars, which may present several anatomical variations, have the highest frequency of endodontic treatment. The most frequent mesial root canal configuration in the first mandibular molar is type IV (46.2%), followed by type II (16.3%). In the distal canal, type I was found in 57% of cases, followed by V (27%) 8 . Another study on distal canals found 88.6% type I and other atypical configurations 9 . Despite the anatomical correlation between teeth, variations may occur, making it necessary to investigate their internal morphology. The clinician needs to be attentive to the presence of additional canals or configurations of the main root canals to avoid incomplete and inefficient shaping and disinfection that could lead to potential failure of endodontic treatment 7 , 10 .
Cone Beam Computed Tomography (CBCT) can be used to assess anatomical aspects in vivo . Its main advantage over periapical radiographs is that it provides three-dimensional visualization of the tooth and can avoid superimposition of anatomical structures, enabling important aspects of internal tooth anatomy, such as the number of roots and especially root canals, to be visualized with better definition 11 . The study of internal anatomy is very important to the clinician. To date, no study has compared all these tooth groups in the same patient. Therefore, the aim of this study was to use CBCT scans to analyze the morphology and anatomical symmetry of molars, premolars, and mandibular incisors.
MATERIALS AND METHOD
This study was approved by the Sao Leopoldo Mandic Research Institute ethics committee through protocol #5.771.849. It was an observational study using images from CBCT scans to evaluate the morphology and symmetry of the roots and root canal systems of molars, premolars and mandibular incisors of patients from a multiracial subpopulation in southern Brazil for whom examinations had been requested for other purposes not related to this research. G*Power 3.1 software 12 was used to calculate the sample size. To test the difference in the number of canals in molars, premolars, and mandibular incisors in relation to symmetry (right side vs. left side), a sample size of 52 paired teeth was estimated for each of the three analysis groups, considering the use of a two-sided test, a small effect size (ES) (d = 0.40 Cohen, 1992), a power of 80%, and a 95% confidence level.
A total 45 CBCT scans of the mandibular region were analyzed, with 444 teeth evaluated: 120 molars, 148 premolars and 176 mandibular incisors. The study included exams from the mandibular region from patients aged from 18 to 60 years old. Inclusion criteria were teeth with complete root development, no endodontic treatment, no evidence of root fracture, no intrarradicular retainers and no prosthetic crowns, no root resorption, and no calcifications. Exclusion criteria were images that did not meet quality standards and patients younger than 18 years.
CBCT images were acquired with a Vatech American (North South, Fort Lee, United States) Pax I3D Smart Pht 30 LFO CT scanner using the following acquisition protocol: *voltage 100-240 V and 2.2 Kva mA, FOV 100*85 voxel 10. MA and minimum exposure time 18 seconds.
The three-dimensional images were evaluated in a darkroom using the DICOM viewer HOROS, iCat Solutions Ltd, , Norwich, United Kingdom. The evaluation started with the number of roots, followed by the analysis of the number and configuraron of canals on the axial plane, followed by the sagittal and finally the coronal plane. For each group of teeth, the following information was recorded: gender, number of roots, number of canals, SCR configuraron according to Vertucci’s classification ( Fig. 1 ), and whether there was symmetry between each subject’s right and left homologous teeth.
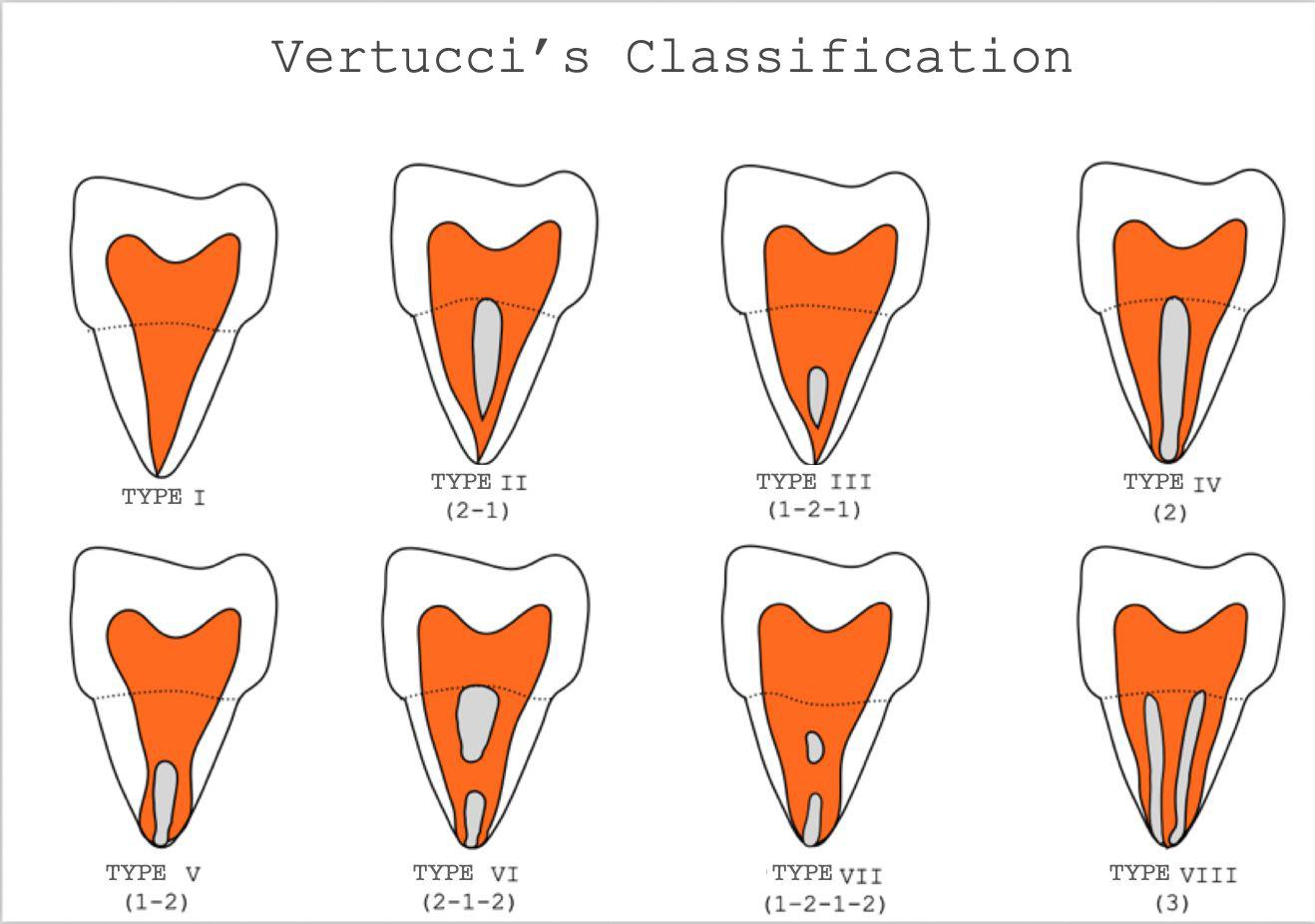
Fig. 1 Vertucci’s classification. Type I: a single canal exits the pulp chamber and extends to the apex; type II: two canals leave the pulp chamber separately and unite into a single canal anterior to the apex; type III, a single canal leaves the pulp chamber, divides into two in the middle third, and unites into a single canal in the apical third; type IV, two canals leave the pulp chamber and extend to the apex; type V, a single canal leaves the pulp chamber and divides into two canals with two separate foramina; type VI, two canals exit the pulp chamber, reunite in the root body, and divide again into two separate canals at the apex; type VII, a single canal exits the pulp chamber, divides into two, then reunites into one canal and terminates in two separate canals; type VIII, three separate canals exit the pulp chamber and extend to the apex.
Statistical analysis
Image analysis was performed by two experienced calibrated examiners (an endodontist and a radiologist). The Kappa agreement test showed perfect agreement between the two examiners for all tooth groups examined (Kappa = 1.00; 95% CI: 1.00-1.00) and near-perfect agreement regarding the number and configuration of the root canal system. Descriptive statistics were performed with frequencies and percentages of categorical variables. To test whether sex and side variables were associated to the number of roots, number of canals, and Vertucci classification, the chi-square test (X2) or Fisher’s exact test was used, as appropriate. Effect size was scored according to Cramer’s V, using the following classification: small < 0.30; moderate 0.30-0.49; large > 0.50. Analyses were performed using SPSS software (IBM SPSS Statistics, version 22.0; IBM Corporation). A p-value < 0.05 was assumed for statistical significance.
RESULTS
A total 444 teeth were assessed: 120 molars (60 F and 60 M), 148 premolars (73 F and 75 M), and 176 mandibular incisors (91 F and 85 M). No statistically significant difference was found in the number of roots in incisors, premolars and molars between men and women (p < 0.05).
Table 1 Comparison of absolute frequencies (percentages) of the number of canals in incisors, premolars and molars for males and females
| Tooth | Sex | Number of canals | X 2 | p-valor | ES | ||||
|---|---|---|---|---|---|---|---|---|---|
| 1C | 2C | 3C | 4C | 5C | |||||
| Central incisor | F | 37(82%) | 8(18%) | - | - | - | 3.019 | 0.08 | 0.19 |
| M | 27(66%) | 14(34%) | - | - | - | ||||
| Lateral incisor | F | 38(83%) | 8(17%) | - | - | - | 4.139 | 0.04* | 0.21 |
| M | 28(64%) | 16(36%) | - | - | - | ||||
| 1st premolar | F | 28(74%) | 10(26%) | - | - | - | 0.358 | 0.55 | 0.07 |
| M | 27(67%) | 13(33%) | - | - | - | ||||
| 2nd premolar | F | 35(100%) | 0(0%) | - | 1.00 | 0.12 | |||
| M | 34(97%) | 1(3%) | |||||||
| 1st molar | F | - | - | 14(48%) | 15(52%) | - | 0.488 | 0.48 | 0.09 |
| M | - | - 15(58%) | 11(42%) | - | |||||
| 2nd molar | F | - 6(19%) | 24(77%) | 1(3%) | 0(0%) | 5.340 | 0.08 | 0.29 | |
| M | - | 1(3%) | 31(91%) | 1(3%) | 1(3%) | ||||
Table 2 Comparison of the absolute frequencies (percentages) of the number of roots found in the inci-sors, premolars, and molars on the right and left sides
| Tooth | Side | Number of roots | p-valor | ES | ||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | ||||
| Central incisor | R | 43(100%) | - | - | - | - |
| L | 43(100%) | - | - | |||
| Lateral incisor | R | 45(100%) | - | - | - | - |
| L | 45(100%) | - | - | |||
| 1st premolar | R | 37(97%) | 1(3%) | - | 1.00 | 0.004 |
| L | 39(98%) | 1(2%) | - | |||
| 2nd premolar | R | 33(100%) | - | - | - | - |
| L | 36(100%) | - | - | |||
| 1st molar | R | - | 25(96%) | 1(4%) | 0.47 | 0.14 |
| L | 29(100%) | 0(0%) | - | |||
| 1nd molar | R | 2(6%) | 29(91%) | 1(3%) | 0.80 | 0.13 |
| L | 2(6%) | 31(94%) | 0(0%) | |||
Table 3 Comparison of absolute frequencies (percentages) of the number of canals found in incisors, premolars and molars on the right and left sides
| Tooth | Side | Number of canals | X 2 | p-valor | ES | ||||
|---|---|---|---|---|---|---|---|---|---|
| 1C | 2C | 3C | 4C | 5C | |||||
| Central incisor | right | 32(74%) | 11(26%) | - | - | - | <0.001 | 1.00 | 0.00 |
| left | 32(74%) | 11(26%) | - | - | - | ||||
| Lateral incisor | right | 33(73%) | 12(27%) | - | - | - | <0.001 | 1.00 | 0.00 |
| left | 33(73%) | 12(27%) | - | - | - | ||||
| 1st premolar | right | 28(74%) | 10(26%) | - | - | - | 0.358 | 0.55 | 0.07 |
| left | 27(67%) | 13(33%) | - | - | - | ||||
| 2nd premolar | right | 33(100%) | 0(0%) | - | - - | 0.930 | 0.33 | 0.12 | |
| left | 35(97%) | 1(3%) | - | - - | |||||
| 1st molar | right | - | - | 13(50%) | 13(50%) | - | 0.147 | 0.70 | 0.05 |
| left | - | - | 16(55%) | 13(45%) | - | ||||
| 2nd molar | right | - | 3(9%) | 27(85%) | 2(6%) | 0(0%) | 2.763 | 0.58 | 0.22 |
| left | - | 4(12%) | 28(85%) | 0(0%) | 1(3%) | ||||
The number of canals did not differ significantly between males and females, except in lateral incisors, where a higher proportion of teeth with two canals was observed in males than in females ( Table 1 ) (P < 0.05).
Comparison of the right and left sides showed no statistically significant differences in number of roots ( Table 2 ) or number of canals ( Table 3 ) in incisors, premolars and molars (p < 0.05). According to Vertucci’s classification, Type I was the most frequent in mandibular incisors and premolars. In central incisors, Type I was found in 82% of females and 66% of males. In lateral incisors, Type I was found in 83% of females and 64% of males. In first mandibular premolars, Type I was found in 74% of females and 73% of males, while in second mandibular premolars, the percentages were 100% for females and 97% for males ( Table 4 ).
In molars, several Vertucci types were observed. In first molar mesial roots, the most frequent was type IV (59% for females and 65% for males), followed by type II (41% for females and 35% for males). In distal roots, type I was the most prevalent (52% for females and 65% for males), followed by type II (21% for females and 19% for males), type III (17% for females and 4% for males), and type V (10% for females). For the second mandibular molars, a high percentage of type II was found in mesial roots (52% for females and 51% for males), followed by type IV (26% for females and 43% for males), while types I, III, and V were found in lower frequencies.
The distal canal was type I in most cases (97% for both females and males) ( Table 4 ).
The Vertucci frequencies on the right and left side can be found in Table 5 .
DISCUSSION
This observational study analyzed CBCT scans ofthe mandible of men and women from a subpopulation in southern Brazil. Radiographic analysis is essential in endodontics for diagnosis, treatment planning and implementation, and preservation. Periapical radiography is the most important complementary examination. However, it has some limitations, such as compression of anatomical structures, conversion of three-dimensional structures into two-dimensional, and possible overlap of anatomical structures that may obscure the area of interest. CBCT provides a detailed, three-dimensional assessment of teeth and aids in diagnosis, planning, treatment, and follow-up after endodontic therapy 13 . In the present study, a single root was detected in 100% of the cases in central and lateral incisors, which agrees with the studies by Valenti-Obino et al. 14 and Sroczyk-Jaszczynska et al. 15 , in which 978 and 420 mandibular incisors were analyzed, respectively. Regarding the number of canals, a higher frequency of a single canal was observed in females (82% in central incisors and 83% in lateral incisors) than in males (66% in central incisors and 64% in lateral incisors). However, in absolute frequency, these data were 74% with one canal and 26% with two canals in central incisors, and 73% with one canal and 27% with two canals in lateral incisors. Similar data were reported in the study by Sroczyk-Jaszczynska et al. 15 , where the frequency of a single canal was about 65% in central incisors and 67% in lateral incisors, while the frequency of two canals was about 33% in central incisors and 31.76% in mandibular lateral incisors.
Table 4 Comparison of the absolute frequencies of the Vertucci scale in incisors, premolars and molars between males and females
| Tooth | Root | Side | Vertucci scale | p-value | |||||
|---|---|---|---|---|---|---|---|---|---|
| I | II | III | IV | V | VI | ||||
| Central incisor | B | right | 32(74%) | 3(7%) | 8(19%) | - | - | - | 1.00 |
| left | 32(74%) | 3 (7%) | 8(19%) | - | - | - | |||
| L | right | - | - | - | - | - | - | - | |
| left | - | - | - | - | - | ||||
| Lateral incisor | B | right | 33(74%) | 6(13%) | 6(13%) | - | - | - | 0.92 |
| left | 33 (73%) | 5(12%) | 7(15%) | - | - | - | |||
| L | right | - | - | - | - | - | - | - | |
| left | - | - | - | - | - | ||||
| 1st premolar | B | right | 29(76%) | - | 4(11%) | - | 5(13%) | - | 0.67 |
| left | 28(70%) | - | 7(18%) | - | 5(12%) | - | |||
| L | right | 1(100%) | - - - - - | - | |||||
| left | 1(100%) | - - - - - | |||||||
| 2nd premolar | B | right | 33(100%) | - - - - | 0(0%) | 0.33 | |||
| left | 35(97%) | - - - - | 1 (3%) | ||||||
| L | right | - - - - - - | - | ||||||
| left | - - - - - - | ||||||||
| 1st molar | M | right | - | 8 (31%) | - | 18(69%) | - | - | 0.28 |
| left | - | 13(45%) | - | 16(55%) | - | - | |||
| D | right | 14(54%) | 7(27%) | 3(11%) | 1(4%) | 1(4%) | - | 0.77 | |
| left | 18(62%) | 4(14%) | 3(10%) | 2(7%) | 2(7%) | - | |||
| 2nd molar | M | right | 2(6%) | 18(56%) | 2(6%) | 9(28%) | 1(4%) | 0(0%) | 0.55 |
| left | 2(6%) | 15(47%) | 0 (0%) | 13(41%) | 1 (3%) | 1(3%) | |||
| D | right | 30(97%) | - | 1(3%) | - | 0(0%) | - | 0.37 | |
| left | 30(97%) | - | 0(0%) | - | 1(3%) | - | |||
Table 5 Comparison of the absolute frequencies of the Vertucci scale in incisors, premolars and molars on the right and left sides
| Tooth | Root | Side | Vertucci scale | p-value | |||||
|---|---|---|---|---|---|---|---|---|---|
| I | II | III | IV | V | VI | ||||
| Central incisor | B | right | 32 (74%) | 3 (7%) | 8 (19%) | - | - | - | 1.00 |
| left | 32 (74%) | 3 (7%) | 8 (19%) | - | - | - | |||
| L | right | - | - | - | - | - | - | - | |
| left | - | - | - | - | - | ||||
| Lateral incisor | B | right | 33 (74%) | 6 (13%) | 6 (13%) | - | - | - | 0.92 |
| left | 33 (73%) | 5 (12%) | 7 (15%) | - | - | - | |||
| L | right | - | - | - | - | - | - | - | |
| left | - | - | - | - | - | ||||
| 1st premolar | B | right | 29 (76%) | - | 4 (11%) | - | 5 (13%) | - | 0.67 |
| left | 28 (70%) | - | 7 (18%) | - | 5 (12%) | - | |||
| L | right | 1 (100%) | - | - | - | - | - | - | |
| left | 1 (100%) | - | - | - | - | - | |||
| 2nd premolar | B | right | 33 (100%) | - | - | - | - | 0 (0%) | 0.33 |
| left | 35 (97%) | - | - | - | - | 1 (3%) | |||
| L | right | - | - | - | - | - | - | - | |
| left | - | - | - | - | - | - | |||
| 1st molar | M | right | - | 8 (31%) | - | 18 (69%) | - | - | 0.28 |
| left | - | 13 (45%) | - | 16 (55%) | - | - | |||
| D | right | 14 (54%) | 7 (27%) | 3 (11%) | 1 (4%) | 1(4%) | - | 0.77 | |
| left | 18 (62%) | 4 (14%) | 3 (10%) | 2 (7%) | 2 (7%) | - | |||
| 2nd molar | M | right | 2 (6%) | 18 (56%) | 2 (6%) | 9 (28%) | 1 (4%) | 0 (0%) | 0.55 |
| left | 2 (6%) | 15 (47%) | 0 (0%) | 13 (41%) | 1 (3%) | 1 (3%) | |||
| D | right | 30 (97%) | - | 1 (3%) | - | 0 (0%) | - | 0.37 | |
| left | 30 (97%) | - | 0 (0%) | - | 1 (3%) | - | |||
Regarding canal configuration according to Vertucci’s classification, it was found that mandibular incisors were more frequently types I, II and III. Types I and III were even more prevalent for central incisors and types I (83%) and III (13%) for lateral incisors in females, and I (64%) and II (20%) in males, with statistical difference between the groups. Somewhat different data were reported by Valenti-Obino et al. 14 , who found type I canals in 57% of mandibular lateral incisors and 55% of mandibular central incisors, type II in 35.7% and 34.3%, and type III in 9.3% and 6.9%. In this study, type IV and VII configurations were also found, although these differences can be explained by the sample size.
Regarding symmetry between the right and left sides of the same group of teeth, it was observed that females had higher symmetry than males. Symmetry of central and lateral incisors was present in 100% of females, while in males, symmetry was 85% for central incisors and 91% for lateral incisors. Similar data were reported by Sroczyk-Jaszczyñska et al. 15 , who found symmetry in 100% of mandibular incisors, while Valenti-Obino et al.14found symmetry in 44.6% of central incisors and 44.8% of lateral incisors.
One- and two-rooted premolars were found: 100% of female patients had a single root in both first and second premolars, while two (5%) teeth with two roots were observed in first premolars in males. Similar data were found by Alfawaz et al.16in a sample of 377 mandibular first premolars, of which 97.5% of female and 95.2% of male first premolars were found to have a single root. In terms of absolute data, a frequency of 97% first premolars with a single root and 100% second premolars with two roots were observed in this study.
Regarding the number of canals and canal configuration according to Vertucci’s classification, more teeth with one canal than with two were observed. In second premolars, the most common configuration was Type I (100% in females and 97% in males), while only one type VI (3%) was found. In first premolars in females, 74% had type I configuration, 18% type III and 8% type V. Different data were reported by Alfawaz et al. 16 , where the frequency of type I was 87.8%, type II 3.4%, and type V 1.5%; other configurations were also found (types IV and VIII). In males, the current study observed a higher frequency of type I (73%), type III (10%) and type V (17%), in contrast to the data of Alfawaz et al. 16 , who found the occurrence of type I in 88.2%, type II in 3.8%, type III in 2.2%, type IV in 3.8%, type V in 6%, and type VI in 0.5% in male patients.
Symmetry was found in 84.2% of first premolars and in 96.6% of second premolars. These data are similar to those of Alfawaz et al. 16 , where symmetry was found in 96.7% of male patients and 97.3% of female patients.
Molars were found with one, two and three roots. In first molars, two roots were the most common (98%) and only one case with three roots was found on the right side. In second molars, there was one root in 6% of cases, two roots in 92.5%, and three roots in only one case of a second molar on the right side. Similar data were found by Kantilieraki et al. 17 , where in a sample of 478 first molars and 524 second molars, the presence of two roots was observed in 96.44% of first molars and 82.82% of second molars, with second molars being considered the teeth with the greatest variation in both canal configuration and morphology and symmetry.
Regarding the number of canals in mandibular first molars, three canals were observed in about 52.5% of cases and four canals in about 47.5% of cases, with two canals in the mesial root and two in the distal root. Different data were found by Plotino et al. 3 in a Greek population, where three canals were found in 69.2% of mandibular first molars and four canals in 21.4%. The current study found greater differences in second molars, with a higher frequency of teeth with three canals (85%), but teeth with two, four, and five canals were also seen. The study by Plotino et al. 3 found similar data, and 87.5% of teeth had three canals, two in the mesial root and one in the lingual root.
Regarding canal configuration according to Vertucci’s classification, a higher frequency of type II (mean 38%) and type IV (mean 62%) was observed in the mesial root of the first molars, in both females and males. Similar data were found in a study by Gambarini et al. 18 , in which mandibular first molars were evaluated, finding in the mesial root a higher frequency of type IV (59%) and type II (41%). In the current study, distal root configurations was more variable, with the most frequent configuration being type I (58.5%), followed by type II, type III in females, while in males, the most frequent was type IV, followed by type V and type III. The study by Kantilieraki et al. 17 found a higher frequency of type I in distal roots (81.7%) in a Greek population. The current study found higher incidence of type II in mesial roots and type I in distal roots (97%) in second molars, in agreement with the study by Kantilieraki et al. 17 , which also found a frequency of type I canal configuration in the distal roots of mandibular second molars.
Female molars were more symmetrical than male molars: 69% symmetry in female first molars and 36% in males, p=0.023, and 80% symmetry in female second molars and 73% in males. In general, symmetry was 54.2% in first molars and 76.7% in second molars. Different data were found in a study by Plotino et al. 3 , which reports a frequency of symmetry of 70.6% in first molars and 81% in second molars. These differences can be explained by the sample size.
Alghamdi and Khalil 19 analyzed the morphology and symmetry of mandibular second premolars using CBCT in a Saudi population and concluded that there are several anatomical variations in the same population, suggesting that further studies should be conducted to investigate root canal anatomy in other regions of Saudi Arabia. Further studies should be conducted to analyze the morphology and symmetry of the incisor, premolar, and mandibular molar canals of the same individual in different populations and subpopulations.
CONCLUSION
As of the date of completion of this work, this is the first in vivo CBCT study investigating the symmetry of homologous teeth considering several teeth groups in the same patient. The present results showed that there was no symmetry between the homologous teeth from the right and left sides, in the same patient, and the teeth showed different morphologies, considering number of roots and the number of canals.

