











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Preservation of renal allograft functions in renal transplant recipients is one of the most important target for prevention of mortality and morbidity and improving patient’s survival rates and quality of life.1-2 However, despite functional renal grafts, the most common cause of mortality in renal transplant patients is still cardiovascular disease (CVD).In addition to classical cardiovascular risk factors, drug related adverse reactions such as post-transplant diabetes, hyperlipidemia, development of arterial hypertension, impaired renal function and proteinuria should be considered. Besides the positive effects of calcineurin inhibitor (CNI) regimens on prevention of rejection, they lead to hypertension, left ventricular hypertrophy and vascular fibrosis and cause negative cardiovascular and renal effects.(3-4) Therefore, the use of antiproliferative inhibitors of m-TOR (mammalian target of rapamycin) (m-TORi) with low-dose CNI, or after cessation of CNI, could being used to prevent CNI side effects.(5-7) It is thought to reduce vascular fibrosis and decrease cardiovascular risk especially with its antiproliferative effects.(8-9)
Urokinase plasminogen activator (uPA) is the primary serine protease (plasminogen activator) involved in vascular remodeling processes(10) and its receptor, soluble urokinase plasminogen activator receptor (SUPAR) is a membrane-linked protein and expressed on various cells. During inflammatory stimulation, cleaved UPAR releases the soluble form, SUPAR, into the circulation. Correlating with proinflammatory markers, SUPAR has been associated with endothelial dysfunction, atherosclerosis, and plaque destabilization. In addition to the cardiovascular patients with cardiovascular problems, some studies shown that there is an association between increasing risk of CVD and general mortality with SUPAR in the general population.(11-12)
Non-immunological factors play a role in renal allograft dysfunction as well as immunological. Dyslipidemia, cardiovascular events, atherosclerosis and chronic renal allograft dysfunction are amongst the non-immunological causes and may adversely affect patient and graft survival.(14) For instance, the use of tacrolimus is thought to play a role in the pathogenesis of chronic allograft dysfunction by causing an increase in oxidized LDL of lipid peroxidation product as known oxidized low-density lipoprotein(ox-LDL).(15)
For defining the effect of the immunosuppressive regimen on the early atherosclerotic markers, we compared SUPAR and Oxidized LDL/LDL as a cardiovascular risk marker in two groups of patients receiving m-TORi or CNI.
MATERIAL AND METHODS
Patient selection
Patients were selected from those followed in our clinic between April 2018 and July 2019. Eighty-three transplant patients between 30-60 years of age were selected.Patients within the first year after transplantation and the first 6 months after switching from CNI to mTORi were included. Patients with GFR below 30 ml/min, history of congestive heart failure were excluded from the study; glomerular filtration rates were calculated using the Modification of Diet in Renal Disease (MDRD).Eligible patients were consecutively selected from our transplantation center according to our study criteria. In our clinic, induction with CNI is chosen as the standart immunosuppressive regimen. In the follow-up, m-TORi was switched to at different times due to low immunological risk, CNI toxicity, skin lesions, gingival hypertrophy, tumor development and uncontrolled diabetes. Could be in this way? Therefore, all of the patients using m-TORi were using CNI from the beginning and were included in our study those who had been swichted to m-TORi for at least 6 months.Drug levels were set to be in the range of 5-8 ng/mL for Tacrolimus, 5-10 ng/mL for sirolimus, and 3-8 ng/mL for everolimus. All patients in the CNI group were receiving tacrolimus.
Thirty five patients were taking CNI(tacrolimus) + MFA + prednisolone, 48 patients were taking mTORi (everolimus-sirolimus) + MFA + prednisolone depending on the immunosuppressive regimen. Routine biochemical parameters, sUPAR level and ox-LDL level were compared between the groups of patients who received m-TORi and CNI.Informed consents were obtained from the patients and blood samples were taken.The blood samples were drawn into serum separator tube (Vacutainer® SST II, Becton Dickinson, USA) from individuals. Serum separator tubes were centrifuged at room temperature for 10 minutes at 1500 g. The serum was separated and stored at -20 C until analysis. Serum suPAR and oxidized LDL levels were analyzed by (Enzyme-Linked ImmunoSorbent Assay) ELISA method (Elabscience® suPAR ELISA, Kit Catalog no. E-EL-H2584 and Oxide-LDL ELISA Kit, Catalog NoE-EL-H0124, USA) and expressed as nanogram per milliliter and picogram per milliliter, respectively.
Statistical analysis
For statistical analysis, the Statistical Package for Social Sciences version 17.0 (SPSS Inc, Chicago, IL) was used. Results were expressed as mean ± standard deviation unless otherwise stated. Variables with non-normal distribution were expressed as mean ± standard error. Between group comparisons of continuous data for two groups were performed using the Student t test or the Mann-Whitney U test when appropriate. The chi-square test with Yates correction and Fisher’s exact test were used for contingency tables for non-numerical data, when appropriate. Correlations between numerical parameters with non-normal distribution were analyzed with Spearman’s rho correlation test. Intra-group comparison of the variables with normal distribution was performed by paired sample T test and variables with non-normal distribution were compared by Wilcoxon test. All tests of significance were two sided, and differences were considered statistically significant when the P value was 0.05 or lower. Since SUPAR and oxLDL values showed abnormal distribution, logarithmic transformation was applied and specified as logSUPAR and log oxLDL. Linear regression analysis was performed to investigate the independent relationship with oxLDL and SUPAR with other clinical parameters.
Ethics: The study was approved by the local ethical committee.
RESULTS
Baseline demographic data showed no difference between patients using m-TORi and those using CNI, except the duration since transplantation.Patients using CNI had a shorter post-transplant period. (Table 1)
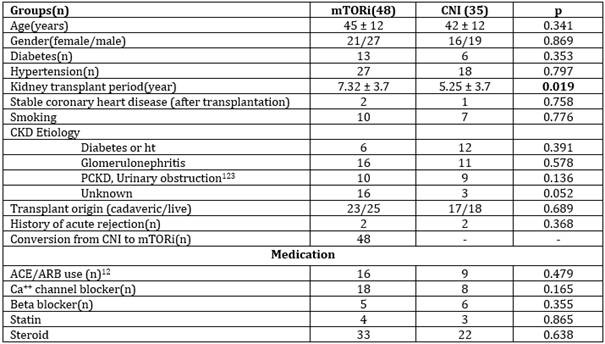
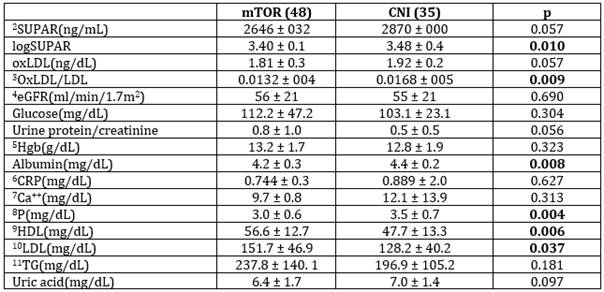
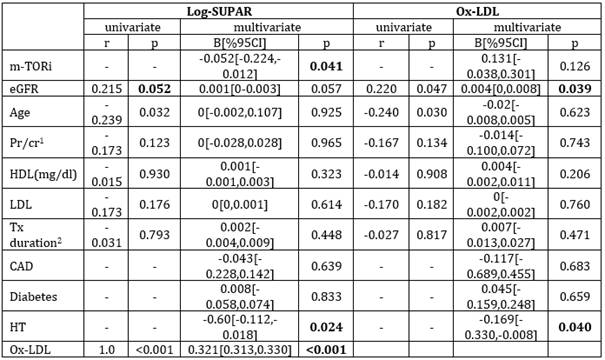
Table 3: Univariate and multivariate analysis of relationship between logSUPAR, ox-LDL and oher variables.
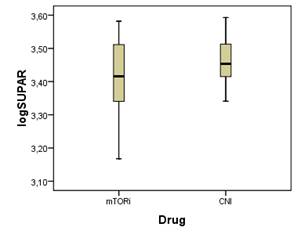
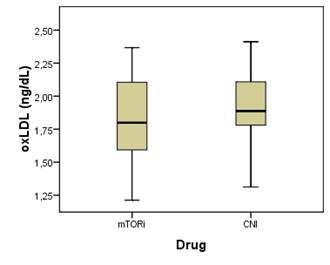
As shown in Figure 1, patients using m-TORi had lower SUPAR levels (2739±736 vs 2830±538,p=0.110), but did not reach statistical significance. Because of SUPAR levels showed abnormal distribution features, when logarithmic transformation was applied, log-SUPAR values were lower in the group receiving m-TORi (3.40 ± 0.1 vs 3.48 ± 0.4, p=0.010) Although there was no difference between ox-LDL(1.81 ± 0.3 vs 1.92 ± 0.2, p=0.091) levels, oxLDL/LDL levels were higher(0.0168± 005 vs 0.0132 ±004, p=0.009) in the CNI group. Protein/creatinine ratios in spot urine were higher in the group receiving m-TORi but were not statistically significant (p=0.056). Serum albumin levels were lower in the group receiving m-TORi (4.2 ± 0.3 vs 4.4 ± 0.2, p=0.008).Patients using m-TORi had lower phosphate levels (3.0 ± 0.6 vs 3.5 ± 0.7, p=0.004), high HDL (56.6 ± 12.7 vs 47.7 ± 13.3, p=0.006) and low LDL (151.7 ± 46.9 vs 128.2 ± 40.2, p=0.037) .
Correlation analysis showed negative correlation between age and log-SUPAR (r=-0.239, p=0.032) and ox-LDL (r=-0.240, p=0.030) levels.A weak correlation between eGFR and log-SUPAR (r=0.215, p=0.052) and strong correlation between ox-LDL (r=0.220, p=0.047) were found.In linear regression analysis, a statistically significant relationship was detected between the use of m-TOR and log-SUPAR (β=-0.052, 95% CI [-0.224, -0.012], p=0.041). eGFR was poorly associated with log-SUPAR(p=0.057) however it was independently and significantly associated with ox-LDL (β=0.004, 95% CI [0.0.008], p=0.039). A negative and independent relationship was found between HT and log-SUPAR (β=-0.60, 95% CI--0.112, -0.018], p=0.0024) and ox-LDL (β=-0.169 [-0.330, -0.008], p=0.040). In addition to these very strong correlations (r=1.0, p <0.001), an independent relationship(β=0.321 [0.313,0.330], p<0.001) was detected between ox-LDL and SUPAR.
DISCUSSION
One of the aspects of immunosuppressive drug usage in kidney transplantation is increasing cardiovascular problems. The adjustment of immunosuppressive therapy in kidney transplant recipients (KTRs) for different risk factors is a challenging condition. Among standard triple immunosuppressive regimens (tacrolimus+MPA+prednisolone), tacrolimus, a CNI, is considered to be the most effective prophylactic agent for graft rejection; however, it is also believed to cause hypertension and vascular intimal fibrosis leading to increased nephrotoxicity and cardiovascular disease, especially with high doses in the long term. Everolimus belongs to a class of immunosuppressive drugs called m-TORi; they are well known for their antiproliferative effects that make everolimus a good candidate to be used in drug eluting coronary stents. In experimental animal models m-TORi have shown a beneficial effect in slowing progression of atherosclerosis, decreasing lipid deposition in atherosclerotic plaque and promoting plaque stability.(17-18) Multiple clinical studies have demonstrated that m-TORi may reduce the incidence and severity cardiac allograft vasculopathy.(19-20) Studies on kidney transplantation are directed to the protective effects of m-TORis against arterial distensibility, hypertension and left ventricular hypertrophy and this topic should be further supported by studies.(21-22)In our study, we documented the vascular protective effects of m-TORi at molecular level.In previous studies, suPAR has found to be associated with endothelial dysfunction, atherosclerosis and plaque destabilization. In our study, log-SUPAR values were lower in the group receiving m-TORi (3.40 ± 0.1 vs 3.48 ± 0.4, p=0.010). This finding supports previous clinical studies.
Spot urine protein / creatinine ratio (0.8 ± 1.0) was higher in the group receiving m-TORi (0.5± 0.5) but did not reach statistically significant level (p: 0.056) in m-TORi group. As well known before, m-TORi cause proteinuria(22) our findindg are compatible this information,
In numerous preceding studies, SUPAR levels were found to be high in proteinuria, especially with primary focal segmental glomerulosclerosis (FSGS).(23-24) However, there are also studies showing that the diagnostic value is low as SUPAR levels increase in various conditions such as membranous disease, minimal change disease, chronic renal failure, and diabetes.(25-26) In our study, there was no difference between log-SUPAR level and proteinuria (p=0.965).
Various studies have demonstrated dyslipidemia to occur more frequently in patients on m-TORi compared with those administered CNIs. Tedesco Silva and Pascual showed a grater prevalence of hypercholesterolemia in patients under everolimus treatment and demonstrated that total cholesterol and triglyceride levels were lower in patients on standard CNI therapy in ASCERTAIN trial.(27) However, despite hyperlipidemia, m-TORi cause a decrease in cardiovascular risk, as shown in multiple studies.(28-29)In our study, we found higher HDL levels in patients using m-TORi than compared to those using CNI (56.6 ± 12.7 mg/dl vs 47.7±13.3, p=0.006).In addition, we found oxidized LDL with proven cardiovascular adverse effects to be lower in the m-TORi group, although it did not reach statistical significance (1.81 ± 0.3, p=0.057). Ox-LDL/LDL ratio was found lower in patients using m-TORi with high statistical significance (0.0132 ± 004, p=0.009). In order to avoid CNI toxicity, further investigation is warranted considering the increased risk of rejection with m-TORi and the increased level of metabolic risk factors associated with high doses of steroids associated with m-TORi.
In our study, the CNI group was younger and the frequency of HT-DM was lower. This is probably because patients who developed DM and uncontrolled HT after the initiation of immunosuppression with CNI are switched to m-TORi.
LIMITATIONS
Our study is not randomized and the number of patients is small. Therefore, it is difficult to establish a link between the immunosupressive regimen and increased cardiovascular risk as a result of high SUPAR and ox-LDL levels.Randomized studies are needed on this subject.
CONCLUSION
In our study, m-TORi seem to be superior to CNI in terms of cardiovascular risk markers such as ox-LDL and SUPAR levels andhigh SUPAR and ox-LDL levels in the CNI group indicate high cardiovascular risks. If the immunological risk is low in patients with high cardiovascular risk, mTORi can be used.
Conflict of interest: Authors declare no conflict of interest.

