











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
In December 2019, the world faced a new corona virus (SARS-CoV-2) which caused COVID-19.1 In 2020, as a result of the pandemic, the tuberculosis (TB) control services were interrupted. The World Health Organization (WHO) recorded a reduction in the global number of patients diagnosed and treated for TB and an increase in the number of deaths, for the first time in decades.2,3
COVID-19 can affect people infected or ill with TB before, during or after being cured, facilitating in some cases the transition from latent tubercu lous infection (LTBI) to disease, and also increas ing the possibility of making TB evolution more severe due to a higher extension of pulmonary lesions.3-5
It has been proven that people with TB have higher risk of death from COVID-193 and that the use of corticosteroids both for the acute phase and for post COVID-19 organizing pneumonia can lead to TB reactivation.1,2,5 It has also been observed that the “unfavorable” evolution of COVID-19 implies a higher risk of progression from LTBI to active TB.6
Even though information is still limited, there is growing understanding of the interaction of both diseases, and COVID-19 will probably favor the transition from infection to tuberculous disease, regardless of the severity of its course.7
New research on the molecular and cellular mechanisms of M. tuberculosis and SARS-CoV-2 infections have yielded unexpected similarities regarding the pathogenesis and evolution of the coinfection. Long-term lymphopenia, hyperin flammation, lung tissue injury, and imbalance in CD4+ T-cell subsets associated with COVID-19 could propagate the M. tuberculosis infection and disease progression.1,8
The co-existence of TB and COVID-19 is pre sented in Argentina with undetermined values, and a risk which we can assume has increased.2,9,10
We present three case reports of young patients without relevant comorbidities, with risk factors for LTBI (healthcare personnel, family contact) who were diagnosed with pulmonary TB post mild COVID-19 infection, with outpatient symptomatic treatment (not corticosteroids).
CASE REPORTS
Case N° 1: 25-year-old female, resident doctor. Diagnosis of prolactinoma, medicated with cab ergoline. Claims she doesn’t have any history of allergies, surgeries, or use of toxic substances. No family members or cohabitants with history of TB. Complete vaccination scheme for SARS-CoV-2; BCG (bacille Calmette-Guerin) administered when the patient was a child. She had COVID-19 in May 2021, with mild symptoms of the upper airway (UAW), cephalea, dry cough, anosmia and ageusia; no pulmonary involvement.
After having COVID-19, she still had dry cough, initially associated with post-viral sequelae. In July 2021, she started to have episodes of night sweating, weight loss and occasional sibilance, so she started to use supplementary methods, and the chest X-ray showed cavitary infiltrate in right upper lobe (RUL), with suspicion of pulmonary TB. Respiratory physical examination: crepitant rales in the upper area of the right field and isolated sibilance at auscultation.
August 2021: chest CAT (computed axial tomog raphy) shows condensation with alveolar aspect at the posterior segment of the RUL, identifying small images compatible with caves, the biggest be ing 8 mm (Figure 1). Laboratory: high erythrocyte sedimentation rate, negative viral serology. Diag nostic fibrobronchoscopy (FBC) performed with lavage and bronchial biopsy with 3 and 8 BAAR (acid-alcohol-resistant bacillus)/field, respectively, and positive cultures. Patient begins treatment for Category 1 pulmonary TB (unilateral with cave), first phase 2HRZE (isoniazid, H; rifampicin, R; pyrazinamide, Z, and ethambutol, E), and second phase 4HR (isoniazid, H; rifampicin, R), with favorable response.
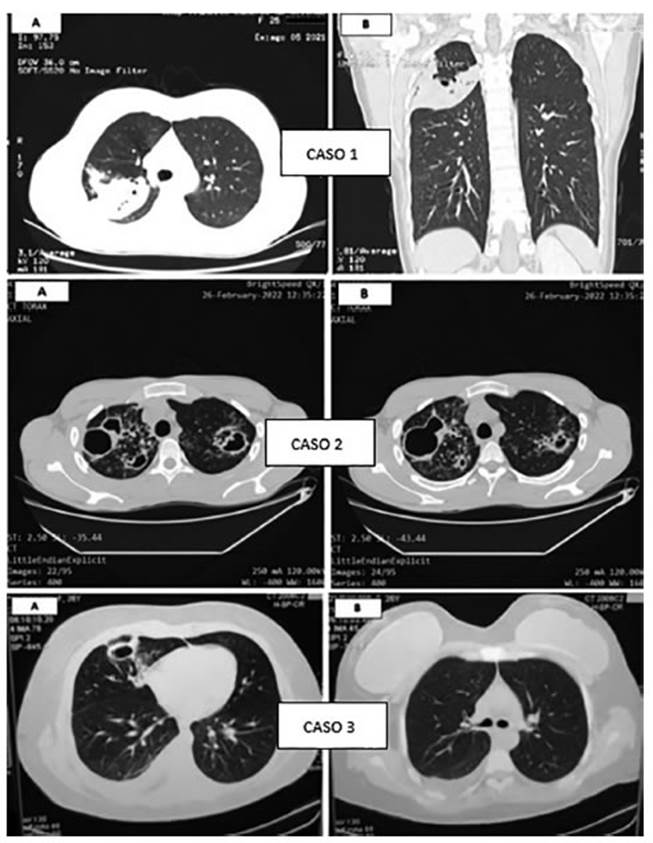
Figure 1 Chest tomography images (lung windows). Case 1: condensation with alveolar aspect at RUL with small cave. Case 2: multiple caves of thick walls in upper fields, as sociated with large tree-in-bud pattern. Case 3: subsegmental linear atelectasis at middle lobe, caves with thick walls and mild pleural effusion.
Case N° 2: 22-year-old male who works at an energy cooperative. No history of diseases, allergies or use of toxic substances. Cohabits with mother, father, and 3 siblings. History of pulmonary TB in the family: the patient’s mother in 2014 (full treat ment), and also the patient’s paternal grandfather and uncle. Complete vaccination scheme for SARS-CoV-2; BCG administered when the patient was a child. He had COVID-19 in April 2021, without respiratory symptoms.
Since May 2021, after COVID-19, he’s been having cough and mucous expectoration, occasion ally mucopurulent (not hemoptoic), dyspnea on exertion, and weight loss. Makes several medical consultations and uses different antibiotic regi mens without symptom improvement. Respiratory physical examination: rhonchus and movement of secretions with coughing.
February/March 2022: chest CAT shows mul tiple caves of thick walls predominant in upper fields, associated with large tree-in-bud pattern and ill-defined opacities with consolidative aspect (Figure 1). Laboratory: high erythrocyte sedimen tation rate, negative viral serology. Sputum for Koch with >10 BAAR/field in two samples. Pa tient begins treatment for Category 1 pulmonary TB (bilateral with cave), first phase 2HRZE and second phase 4HR.
Case N° 3: 26-year-old female, resident doctor. History of obesity class II (BMI: 35). No history of allergies, surgeries, or use of toxic substances. No family members or cohabitants with history of TB. Complete vaccination scheme for SARS-CoV-2; BCG administered when the patient was a child. She had COVID-19 in January 2022 with mild symptoms; no pulmonary involvement.
After having COVID-19, she still had asthenia, and in March she also had fever and cough with mucous expectoration. Respiratory physical exami nation: isolated rhonchus at auscultation.
March 2022: chest CAT shows subsegmental linear atelectasis that affect the medial segment of the right middle lobe, apart from thick caves and mild homolateral pleural effusion (Figure 1). Laboratory: high erythrocyte sedimentation rate, negative viral serology. Negative sputum bacillos copies, positive cultures/GeneXpert® low, without resistance to rifampicin. Patient begins treatment for Category 1 pulmonary TB (unilateral with cave + pleurisy), first phase 2HRZE and second phase 4HR.
DISCUSSION
The presentations of these case reports raise the probable impact of SARS-CoV-2 in the transition from LTBI to disease, excluding the already proven influence of corticosteroids and severe forms of COVID-19. There is increasing evidence to sup port this idea.
TB affects mainly the lungs when the adaptive immune response, mostly performed by T cells, is altered. With coronavirus infection, there is in creased depletion of T cells and a decline in their functional diversity. According to several studies, viruses have been found in T lymphocytes, mac rophages and dendritic cells that can also alter their function. So, the coronavirus infection, which activates cellular immunity, results in the deple tion of the system that is used for fighting TB1.
The significant influence of the SARS-CoV-2 virus on the immune system that produces severe immunosuppression, activation and progression of existing TB foci can modify the tuberculous infec tion due to changes in the nature and intensity of the local cellular immune response. Just like it happens with HIV infections at the AIDS stage, when the reactions of lymphocytes, of epithelioid cells and giant cells become less intense, and in flammation mechanisms and quick dissemination of TB predominate1.
The TB/COVID-19 Global Study Group7 found 71 patients (out of 767) who had been diagnosed with COVID-19 before TB; 48% showed caves, a condition that will likely develop in more than 30 days (time sufficient to develop the disease). Thus, this indirect evidence is against the pre sumption.
A South African study8 showed that COVID-19 didn’t trigger the concomitant activation of CD4+ T cells specific of M. tuberculosis; this is against the hypothesis. However, a significant reduction was found in the frequency of these cells in COVID-19 patients compared to pre-pandemic healthy par ticipants with LTBI. This reduction could affect the host’s capacity to control the infection with M. tuberculosis (latent or new).
There is still a very long way to go, and these questions have been raised. Additional longitu dinal studies that observe patients with TB and COVID-19 over time and compare the proportion of those who acquire the TB disease with a control group without COVID-19 can provide a better understanding of their interaction.7,11
In general, data suggest that TB and COVID-19 are a “cursed duet” and require immediate care7.

