











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
OTB is a severe form of TB. Ocular manifesta tions can be caused by an active infection that invades the eye or by an immunological reaction of retarded hypersensitivity, in absence of the infectious agent. In general, it is secondary to a systemic infection. The most common presenta tions are: chronic anterior uveitis, choroiditis and sclero-keratitis. Given the diagnostic difficulties, the following criteria are used: a) proven: when the bacillus is isolated from an ocular sample, b) probable: isolation in extra-ocular samples, ocular lesions compatible with TB and adequate response to treatment, and c) possible-probable, but without being able to evaluate the evolution.1
In most cases, it isn’t microbiologically con firmed. The general ophthalmologist needs to know the various clinical presentations of TB-related uveitis to timely detect this disease, reduc ing ocular and general morbidity.2
CASE REPORT
3-year-old girl. Creole ethnic group. Comes from the town of La Matanza.
The patient comes for consultation because she had been having fever for the last 15 days, with two to three recorded fever episodes per day (38-39 °C), and dry cough.
Personal history: left lung pneumonia treated as outpa tient, 3 months before admission. Chest X-ray not available.
Family history: TB in a bacilliferous, diabetic uncle undergoing treatment with whom the patient has been cohabiting for 4 months. No contact testing has been done.
Physical examination on admission
Regular general condition. Eutrophic. Febrile. Bacillus Calmette-Guérin (BCG) vaccine c/c. Serum and mucosal rhinitis, dry cough. Tachypnea. Global reduction of air intake, with scarce bilateral fine sub crepitant rales. Ten dency to fall asleep.
Analytical data on admission
Normal blood count. Erythrocyte sedimentation (globular sedimentation rate, GSR): 35/mm3 (1st. hr). Negative blood cultures (BC) (x2). Renal and liver function, coagu lation profile, proteinogram, and immunoglobulins (Ig), all normal.
Nasopharyngeal secretions viral testing (NPST) through indirect immunofluorescence (IIF): isolated Rhinovirus.
Cerebrospinal fluid (CSF): lymphocytic pleocytosis, hypoglycorrhachia. Remaining tests, normal.
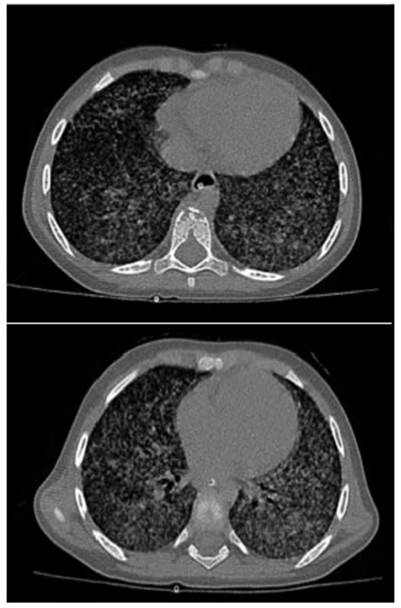
Chest X-ray: micronodular infiltrate with predominant right hemithorax. (Figure 1)

Evolution
The patient remained hospitalized at the Hospital Posadas, with the following tests requested: a) tuberculin test: PPD (purified protein derivative) RT 23 (2TU): 0mm; b) gastric lavage (GL): negative Ziehl Neesel (ZN) and positive cul ture (C) for Mycobacterium tuberculosis (MT); c) serology for human immunodeficiency virus (HIV), hepatitis (A, B, C), toxoplasmosis, herpes simplex virus, syphilis (VDRL, venereal disease research laboratory), chagas Mycoplasma pneumoniae: all negative; d) nuclear magnetic resonance of the brain: normal; f) chest high-resolution computed axial tomography (HRCT): pathological; and g) fundoscopic exam: infiltrates at posterior pole compatible with miliary TB in both eyes. Pupils with clear, well-defined borders. (Figure 2)
Due to clinical symptoms, family history and supple mentary tests, the condition was assumed as disseminated pulmonary TB with pulmonary (miliary), ophthalmic and central nervous system (CNS) involvement. Negative focus control test.
Indicated treatment: ceftriaxone 100 mg/kg/day. Iso niazid (H) 10 mg/kg/day, rifampicin (R) 15 mg/kg/day, pirazinamide (Z) 25 mg/kg/day, ethambutol (E) 20 mg/kg/ day. Meprednisone 1 mg/kg/day, with progressive reduction in 30 days.
The CSF report showed direct common germs and nega tive culture. Negative ZN and positive culture. Gene Xpert® (MT/RIF) for MT: not detected. Meningeal TB confirmed.
After 32 days of hospitalization, positive PCR (polymera se chain reaction) for MT. Gene Xpert® (MT/RIF) negative D, and positive C (MT). Resistant to R. Geno Type MTDRsl. No mutations detected in genes gyrA gyarB, which confer resistance to fluoroquinolones in genes, nor in genes rrs and eis, which confer resistance to capreomycin (Cm) and aminoglycosides. Sensitive to: streptomicin (S), E, amikacin (Km), Cm, H and kanamycin (Km).
After finding there was resistance to R, the treatment remained with H, E, Z and levofloxacin (Lfx) 15 mg/kg/day, in accordance with experts’ recommendations. 18 months of treatment suggested.
2 months after the indicated treatment, GL was per formed: negative ZN and C. Ophthalmologic control after 2 months of treatment: macula with normal shine. Vessels of normal caliber. Raised off-white lesions compatible with tuberculous granuloma outside both vascular arcades. (Figure 3)
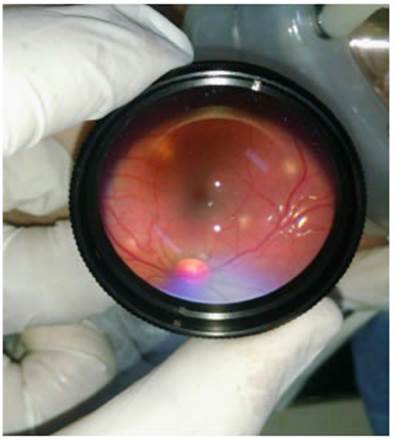
Figure 3 Fundoscopic exam Raised off-white lesions compat ible with tuberculous granuloma outside both vascular arcades.
After 3 months, there was a reduction in the number and size of tuberculous granulomas in both eyes. Attached retina. (Figure 4)
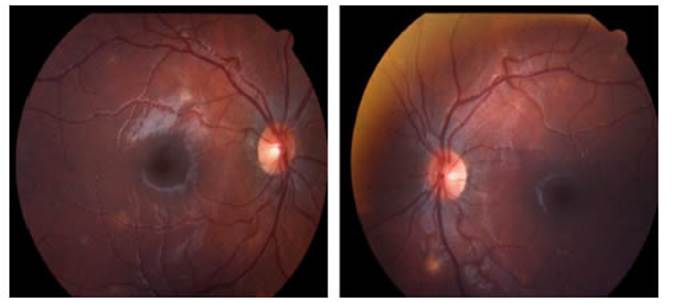
Figure 4 Retinography. Ophthalmic evolution with a reduction in number and size of tuberculous granulo mas in both eyes.
Good clinical evolution. No adverse drug reactions (ADRs). After completing 18 months of treatment, both the chest X-ray and the ophthalmologic examination were normal.
DISCUSSION
TB is an infectious disease produced by Mycobac terium tuberculosis that affects mainly the lungs, but also other organs of the body.
OTB is rare, and its impact is unknown. Accord ing to the regional endemicity of TB, it represents between 0.5% and 18% of the cases of uveitis.3
Children show higher inflammatory response and predisposition to meningeal and miliary TB. In cases of disseminated or miliary TB, it has been described that it represents between 1% and 20%. According to the work of Guadalupe Tenorio et al, the association between miliary TB and ocular involvement accounts for 17.9%.4-6
Within the historical framework, in the study of M. Elena De Benedetti Z et al, the oldest description belongs to Maitre-Jan (1707), who described the case of a patient with a lesion in the iris attributed to TB. Gueneau de Mussy (1830) acknowledged the presence of choroidal tubercula in miliary TB; Manz (1858) described a choroidal tuberculum histologically. The ophthal mologic exam is attributed to von Jaeger (1855), Fraenkel (1867) or Von Graefe and Leber (1868). Cohnheim (1867) provided a detailed description in 7 necropsies and produced choroidal tubercula experimentally. Julius von Michel identified the bacillus in the eye.2,7,8
There is a broad spectrum of clinical presenta tions, which aren’t exclusive to this infectious disease. They vary, depending on the virulence of mycobacteria, the resistance of the host to that mycobacteria, and the degree of tissue hypersen sitivity to it.2,9,10
It can be primary or secondary, unilateral or bilateral. It is caused by an active infection that invades the eye (with the presence of the microor ganism in the ocular tissues) or by an immunologi cal reaction of type IV retarded hypersensitivity to various antigenic components of the mycobacteria itself (in the absence of the infectious agent).
Francisco Infante explains that the ethiopathog eny of the infection can be: a) primary: it occurs through saliva or sputum particles, through soil, dust, detritus of animals or plants that infect the eroded conjunctiva, and b) secondary to blood or lymphatic dissemination. They can both be uni lateral or bilateral.2,4,11
The most common clinical presentations of OTB are: a) uveitis. It can be anterior, intermediate, pos terior or panuveitis. The most common is posterior uveitis (33%-42%), with lesions mostly present in the choroid; b) choroidal granulomas. The choroid receives the highest rate of blood flow and creates an oxygen rich atmosphere that favors the multi plication of bacilli and manifests as focal, multifo cal or serpiginous choroiditis, solitary or multiple choroidal nodules (tubercula), choroidal granu loma (tuberculoma), neuroretinitis, subretinian abscess, endophthalmitis, panophthalmitis and retinal vasculitis; and c) sclero-keratitis.2,6,12-14.
The ophthalmologic exam detects choroidal tubercula, which can be one of the first signs of disseminated disease. Tubercular choroidal granulomas can be solitary or multiple, as those presented in our case. Their size can vary from 0.5 to 3 mm and they are most commonly located at the posterior pole. They have a grey, greyish-white or yellowish color, with ill-defined borders. Vasculitis can be observed, associated with bleed ing and/or exudation in the affected area. When it evolves, the center of the lesion turns pale and the borders become more defined, surrounded by a halo of dark pigment.1,8,9
Other diagnostic and evolution control meth ods: a) fluorangiography and indocyanine green angiography, an up to 100% useful technique to detect choroidal granulomas; b) ecography with variable expressions of the choroidal tuberculoma, which allows us to discard other etiologies such as choroid melanoma and cystic lesions (these methods weren’t used in this case report); and c) optical coherence tomography (OCT) that detects retinal diseases.6
The presence of a positive C-reactive protein (CRP) test at the aqueous or vitreous humor with positive ZN or C, associated with ocular lesion, must be considered a definitive diagnosis. How ever, this rarely happens.
The finding of choroidal tubercula is specific and allows early use of anti-TB therapy, even before the diagnosis is confirmed by other positive samples.
The chest X-ray has good sensitivity to compat ible lesions; HRCT with contrast media can early reveal signs of miliary TB.8,12
Tuberculin hyperergia and/or the histology of caseous granuloma are also illustrative.
Despite the existence of highly sensitive molecu lar tools, the diagnosis of OTB is still probable, and this entity is difficult to detect and difficult to treat. For a diagnosis to be considered as con firmed, the ocular material and the puncture of the aqueous or vitreous humor must be positive for polymerase chain reaction, bacilloscopy or cul ture, or both. Multinational retrospective cohort studies have been organized in an effort to unify nomenclature, diagnosis, and treatment criteria. Global efforts to simplify and standardize the OTB approach could be useful to provide faster and more effective care.12
In our case, the diagnosis was based on the positive epidemiological family history, the images with miliary pattern, the meningeal involvement, the positive bacilloscopy and the abnormal oph thalmologic exam.
Other causes of uveitis with granulomatous lesions in infections are: toxocariasis, toxoplas mosis, syphilis, cat scratch disease, herpes, CMV (cytomegalovirus), histoplasmosis, etc. Also in systemic diseases such as autoimmune diseases or sarcoidosis. Among non-infectious diseases, we must highlight primary and metastatic neoplasia.
Treatment regimens are the same as those for pulmonary TB, but they last longer. We recom mend a fully oral regimen consisting of H, Z, and E for 12 months without using any injectable agent. Longer regimens have the purpose of treating the infection and reducing the antigenic stimulus that is responsible for maintaining retarded immunity. Benedetti et al say that access to infected ocular tissue by the systemic agents is limited by the lack of ocular vascularization. Longer treatments would ensure access by chemotherapeutic drugs, thus avoiding sequelae.2
In certain patients, it is necessary to use sys temic steroids or immunosuppressants to reduce the damage of the hypersensitivity reaction. Severe cases use intravitreal methotrexate. In this case report, corticosteroid therapy was used, due to the meningeal and ophthalmologic components.4
Despite the existence of highly sensitive molecu lar tools, OTB diagnosis is still presumptive. In our case, the diagnosis was based on the positive epidemiological family history, the images with miliary pattern, the meningeal involvement, the positive bacilloscopy and the abnormal ophthal mologic exam.
During evolution, resistance to R was detected. Cases of isolated resistance to R with sensitivity to H are very rare. They represent a problem for the treatment, since there are multiple conditioning factors, experts must be consulted, and a second-line drug resistance test has to be done, rotating the therapeutic regimen for the purpose of obtain ing good evolution, avoiding sequelae, and achiev ing patient recovery. There are several tools to avoid their appearance, one of them being the use of directly observed therapy, avoiding the severe threat they represent for the control of TB.14,15
CONCLUSIONS
OTB is a mycobacterial disease that can go un noticed because it is very rare. It is important to perform routine ophthalmologic exploration in patients with miliary tuberculosis in order to make a timely OTB diagnosis. Bacilloscopy and culture are still essential for the diagnosis of sensitive and resistant TB. The appearance of pharmacological resistance in children implies bad epidemiological control and failure in prevention.

